

Towards a HIPAA Compliant Agentic AI System in Healthcare: A Reference Architecture for Clinical Deployments (2026)




The Health Insurance Portability and Accountability Act was written in 1996, long before large language models, autonomous agents, and Model Context Protocol tool calls existed.
In 2025, the U.S. Department of Health and Human Services updated the HIPAA Security Rule with amendments that explicitly target these new realities — mandating FIPS 140-3 validated encryption, expanding direct Business Associate accountability to any vendor whose infrastructure touches PHI (even transiently, during model inference), and requiring covered entities to inventory every AI system with PHI access as part of an updated risk analysis.
Office for Civil Rights auditors now specifically ask about AI and agent workflows during audits, and a risk analysis that predates a hospital's AI deployment is itself an audit finding.
This changes the design question. The right question is no longer "can I use ChatGPT in my hospital?" It is "how do I architect a governed, agentic AI system that can operate on PHI at scale, prove compliance to an auditor on demand, and evolve as regulations tighten?"
This guide is the answer. It walks through the reference architecture for a HIPAA compliant agentic AI system in healthcare — grounded in the framework proposed by Neupane et al. in the arXiv paper "Towards a HIPAA Compliant Agentic AI System in Healthcare" and extended into the production patterns that actually ship. If you are a CTO, VP of Engineering, health-tech founder, or a hospital innovation leader trying to move from experimentation to governed production, this is your blueprint.
Assistents by Ampcome is the platform we built to embody this architecture, and every principle described here is one we have deployed against in production healthcare environments.
To summarize-
- A HIPAA compliant agentic AI system is one where autonomous, tool-using agents can read, reason over, and act on Protected Health Information (PHI) while enforcing HIPAA's Privacy Rule, Security Rule, and Breach Notification Rule at every step — not just at the vendor-contract layer.
- Standard "wrap ChatGPT, sign a BAA" architectures fail the 2025 HIPAA Security Rule amendments because they cannot demonstrate agent-level chain of custody, minimum-necessary access, or tamper-evident audit trails.
- The reference architecture stands on four pillars: Attribute-Based Access Control (ABAC), a hybrid PHI sanitization pipeline (pre- and post-inference), immutable audit trails, and a semantic governance layer that unifies policy across every agent action.
- Multi-agent orchestration multiplies the compliance surface. Governance has to move up the stack — from the model to the platform.
- Assistents by Ampcome is the production embodiment of this architecture: BAA-ready, on-prem or VPC-isolated, BYOK, model-agnostic, and built around a semantic layer with row-level security and maker-checker approvals native to every workflow.
What Makes an Agentic AI System HIPAA Compliant? (It Is Not the Same as a HIPAA-Compliant Chatbot)
A HIPAA compliant agentic AI system is a software system in which one or more autonomous, tool-using AI agents access, reason over, and take actions on Protected Health Information while satisfying HIPAA's Privacy Rule, Security Rule, and Breach Notification Rule at the architectural, contractual, and operational layers simultaneously. That is a mouthful, so it is worth unpacking why every word matters.
Passive generative AI versus agentic AI.
A passive generative AI chatbot generates text in response to a prompt. It reads, it writes, it does not act. The compliance surface is comparatively narrow: encrypt the prompt in transit, sign a Business Associate Agreement with the model vendor, control who can send prompts, and audit the conversation logs. Agentic AI is a different creature. An agent has tools. It calls APIs. It writes to systems of record. It executes multi-step workflows. It coordinates with other agents. The moment an agent can update a patient's scheduling record, submit a prior authorization, adjust a billing code, or route a message — the compliance surface expands from "reading PHI" to "creating, modifying, and transmitting PHI on behalf of a covered entity." Every one of those actions is a regulated activity under HIPAA.
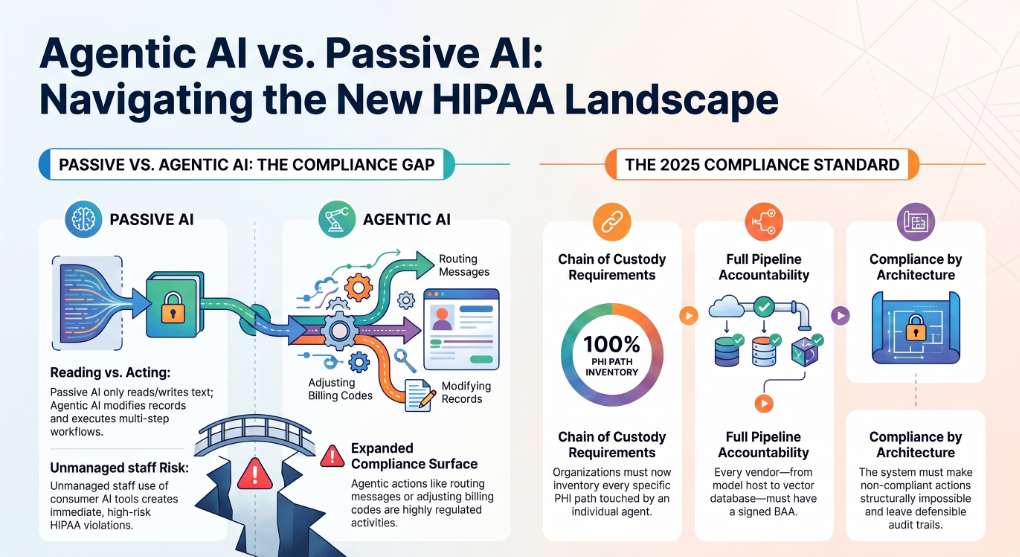
Why the 2025 HIPAA Security Rule amendments matter for agents specifically.
The updated Security Rule closes several gaps that traditional AI deployments have been exploiting. Service account credentials that authenticate a system rather than an agent-level workflow no longer establish chain of custody. Standard TLS implementations without confirmed FIPS 140-3 validation no longer meet the encryption bar. A covered entity's risk analysis is not compliant if it does not inventory every AI agent and the specific PHI paths that agent touches. And direct Business Associate accountability now reaches every vendor in the model inference pipeline — model host, API gateway, vector database, observability platform — each of which must be under a valid BAA if PHI transits their infrastructure.
The shadow AI problem.
In parallel with the regulatory tightening, healthcare organizations are seeing an explosion of "shadow AI" — clinicians pasting deidentified (they hope) case summaries into consumer ChatGPT, back-office staff drafting appeals letters in unmanaged tools, RCM analysts uploading claims spreadsheets to whichever LLM is free. Every one of these interactions is a potential HIPAA violation. The only durable answer is not more policies — it is a governed platform that gives staff the same speed benefit through an approved, compliant channel.
The definition, then, is not one of vendor certifications. It is one of architecture. A HIPAA compliant agentic AI system is one where the architecture makes non-compliant actions structurally impossible, and where every action taken by every agent leaves a defensible trail that satisfies an OCR audit on the first request, not the fifth.
The Reference Architecture — Four Compliance Pillars
The Neupane et al. arXiv paper — the leading academic reference for HIPAA compliant agentic AI — identifies three core compliance mechanisms that every clinical agentic AI system must implement. In production, a fourth pillar becomes non-negotiable: a semantic governance layer that unifies these mechanisms across every agent, every workflow, and every downstream system. Together, these four pillars form the reference architecture.
1. Attribute-Based Access Control (ABAC) — Beyond RBAC
Role-Based Access Control (RBAC) is the traditional healthcare access model — a nurse sees nurse-scoped records, a billing analyst sees billing-scoped records. RBAC is necessary but insufficient when the actor is an autonomous agent. An agent invoked by a scheduling coordinator to confirm an appointment does not need to see the patient's full clinical history — only the demographic and scheduling fields required to complete the task. A blanket "scheduling coordinator" role is over-scoped. This is a direct violation of HIPAA's minimum necessary standard under 45 CFR 164.502(b).
Attribute-Based Access Control solves this by evaluating access dynamically against four dimensions: attributes of the subject (who is the human authorizer, what is the agent identity, what is the invocation context), attributes of the resource (what type of PHI, what sensitivity classification, what patient consent state), attributes of the action (read, write, transmit, delete), and environmental attributes (time of day, location, device posture, workflow phase).
Each request is evaluated against a policy engine that returns an allow or deny decision in real time. Neupane et al. map ABAC directly to Security Rule §164.312(a)(1), and the pattern is now widely adopted in academic reference architectures and in the 2025 HIPAA amendments' expectations.
In production, ABAC without row-level security at the data layer is theatre. Row-level security (RLS) ensures that even if an agent tries to query beyond its scope, the underlying data store refuses to return rows outside the ABAC policy — enforcement is not at the application layer, it is at the SQL layer. This is the pattern the Assistents platform enforces through its semantic layer and governed BI path.
2. Hybrid PHI Sanitization Pipeline (Pre- and Post-Inference)
Every time an agent sends data to a large language model for inference, that data crosses a compliance boundary. Even with a BAA and zero-retention guarantees from the model vendor, sending raw PHI to a model expands the attack surface and violates the principle of defense in depth. The solution is a hybrid PHI sanitization pipeline that sits between the agent and the model.
The pipeline runs in two stages. Pre-inference sanitization intercepts every payload heading to the LLM and redacts PHI using a hybrid approach: deterministic regex patterns for the eighteen HIPAA Safe Harbor identifiers with structured formats (Social Security Numbers, Medical Record Numbers, ZIP codes, phone numbers, dates), combined with a fine-tuned BERT-based clinical Named Entity Recognition model for unstructured contextual PHI (patient names, provider names, facility references in free text). Neupane et al. demonstrate this hybrid approach maps to the Safe Harbor de-identification standard under §164.514(b)(2). The LLM receives only tokenized, minimum-necessary context.
Post-inference re-hydration happens inside a secure workspace after the model returns its response. Redacted tokens are matched back to the original PHI values from a session-scoped, encrypted lookup table, so the final response delivered to the authorized human user is complete and clinically useful. The raw PHI never enters the LLM's context window, and if it did enter (say, through a leak in your sanitization), the audit trail catches it.
This is the pattern that lets an agent draft a discharge summary, summarize a lab panel, or explain a treatment plan without ever exposing patient identifiers to the model — while still delivering the correct, patient-specific output to the clinician. In practice, the sanitization pipeline needs to be model-agnostic, because the models will change and the compliance guarantees cannot.
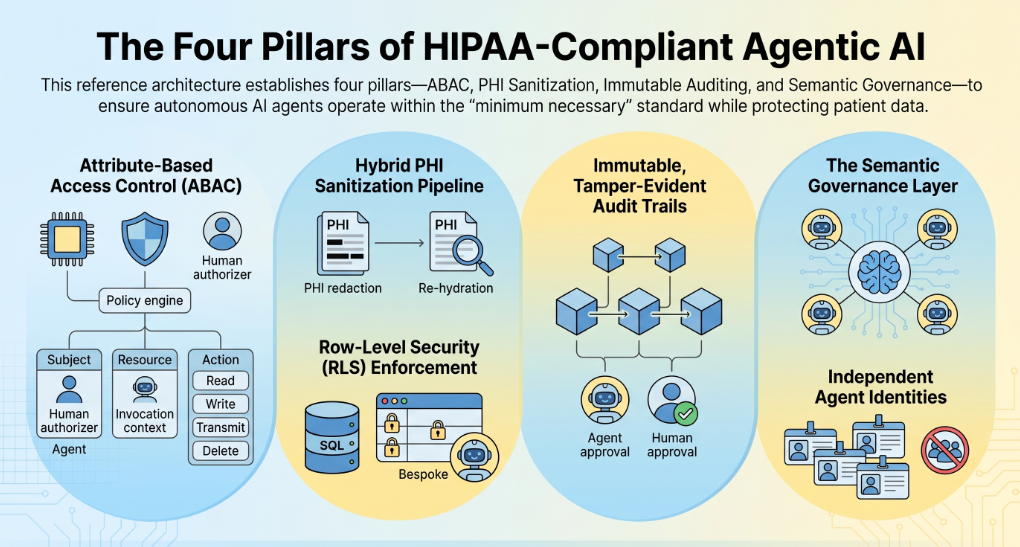
3. Immutable, Tamper-Evident Audit Trails
If an agent acts on PHI, an auditor must be able to answer six questions in seconds, not weeks: who triggered this action, what agent executed it, what PHI was accessed, what reasoning drove the decision, what human approved it (if human approval was required), and what was the final state of the affected record. Every one of those questions maps to a Security Rule requirement under §164.312(b) — the audit-control implementation specification.
An immutable audit trail is one where every agent action is captured with cryptographic write-once semantics, timestamped, sequenced, and streamed into a SIEM the covered entity controls. The record must include the agent's authenticated identity (not a shared service account), the human authorizer who delegated the workflow, the specific operation performed, the exact PHI records accessed, the policy context governing the access decision, the model version and prompt hash used for reasoning, and any human-in-the-loop confirmation that gated the action. Under the 2025 Security Rule amendments, these logs must survive tampering attempts and be delivered to an auditor as an evidence package, not as a discovery investigation.
The "shared service account" pattern is the most common failure here. If every agent authenticates with the same credential and every action logs the same service identity, there is no chain of custody. In a HIPAA compliant agentic AI system, every agent has its own identity, every workflow is bound to a human authorizer, and every log entry carries both.
4. The Semantic Governance Layer — The Missing Fourth Pillar
The three mechanisms above — ABAC, sanitization, and audit — are necessary. They are not sufficient. The gap the academic frameworks do not fully address is what happens when your system runs not one agent, but ten, twenty, or fifty, coordinating on overlapping PHI across dozens of workflows. Every agent needs the same policy definitions, the same metric definitions, the same access decisions, or the system drifts into inconsistency and every drift is a compliance risk.
The semantic governance layer is where you centralize business rules, metric definitions, entity hierarchies, and access policies — and then every agent, every dashboard, every workflow reads from that single source of truth. When a hospitalist program defines "average length of stay" once in the semantic layer, an agent answering a clinician's question, an executive dashboard, and a payer reporting workflow all compute the same number. When a policy says "utilization review analysts cannot see behavioral health notes," the semantic layer enforces it against every agent, every query, every action. This is the layer that turns a collection of compliant agents into a compliant system.
This fourth pillar is what production-grade agentic AI platforms are built around. Assistents.ai's semantic layer is the mechanism that makes ABAC decisions consistent across agents, folds row-scope predicates into every SQL query the platform generates, and keeps metric definitions grounded so BI answers never hallucinate numbers. Governance stops being a set of policies to enforce and becomes a shipping product surface.
The Six Non-Negotiables — Compliance Checkpoints Every Agentic AI System Must Pass
The reference architecture only works if the operational foundation underneath it is sound. Six non-negotiables sit under every HIPAA compliant agentic AI system:
A signed BAA with every vendor that touches PHI, including the model host, the API gateway, the vector database, the observability platform, and any downstream integration. Under the 2025 amendments, direct BA accountability is independently enforceable.
End-to-end encryption meeting FIPS 140-3 requirements — AES-256 at rest, TLS 1.3 in transit, with validated cryptographic modules across every data path an agent touches.
Minimum-necessary access enforced through RBAC and ABAC, with row-level security at the data layer so enforcement is structural, not conventional.
Immutable, tamper-evident audit trails for every agent interaction, exported to the covered entity's SIEM.
Isolated deployment topology — on-premise or VPC-isolated for high-sensitivity workloads. Multi-tenant SaaS deployments with shared inference infrastructure are a structural HIPAA failure regardless of how many certifications the vendor claims.
Automated breach detection and notification workflows that map to the 60-day notification requirement under §164.400–414.
For the operator-facing, enterprise-buyer view of these six — vendor evaluation checklists, BAA negotiation points, and a full procurement framework — see our companion piece: HIPAA-Compliant AI Agents: The Complete Enterprise Deployment Guide (2026). This blog focuses on the architecture; that one focuses on the buying decision.
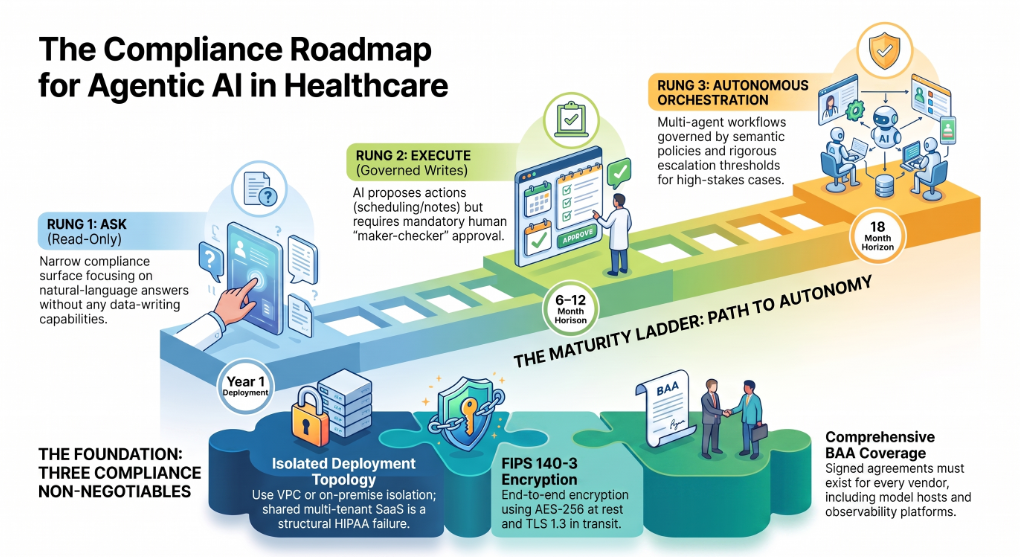
Ask → Execute → Autonomous: A Compliance-Aware Maturity Ladder
Healthcare organizations that jump straight to fully autonomous agents on Day One tend to fail — not because the technology cannot support it, but because their compliance program cannot. A compliance-aware maturity ladder gives you a phased path.
Ask (read-only Q&A over PHI). The narrowest compliance surface. The agent reads governed data, sanitizes the payload, sends it to a model, and returns an answer to a human. No writes, no side effects. Value: instant, natural-language answers to operational questions. Compliance controls needed: ABAC, sanitization, audit. Typical first-year deployment.
Execute (governed writes, updates, and workflows). The agent can now take actions — update a scheduling record, submit a prior authorization draft, route a message, log a note — but only through governed, allow-listed actions with maker-checker approval. Every write is proposed by the AI and confirmed by an authorized human, then re-checked server-side. Compliance controls needed: everything in Ask plus a governed action registry, maker-checker approvals, and expanded audit capture including human confirmation events.
Autonomous (multi-step, cross-system, multi-agent orchestration). The system now runs multi-agent workflows end-to-end — an intake agent captures the patient message, a triage agent routes it, a scheduling agent proposes slots, a follow-up agent confirms. Human oversight shifts from every-action approval to policy-driven escalation for high-stakes cases. Compliance controls needed: everything above plus a semantic governance layer that keeps all agents aligned, cross-agent audit correlation, and rigorous escalation policies for anything above a defined risk threshold.
Most healthcare organizations should be on the Ask rung today, moving to Execute in the six-to-twelve month horizon, and to Autonomous for well-scoped, non-clinical workflows on an eighteen-month horizon. Attempting to jump directly to Autonomous without the semantic governance layer in place is the pattern that produces headline-grade breaches.
Multi-Agent Orchestration Under HIPAA: The Governance Problem No One Is Talking About
Every existing article on "HIPAA compliant AI agents" talks about the challenge as if there is one agent. Production reality is different. A single revenue-cycle workflow may touch an eligibility agent, a coding agent, a prior authorization agent, a claims-status agent, a denial-management agent, and an appeals-drafting agent. A single patient-access workflow may span an intake agent, an insurance-verification agent, a scheduling agent, a reminder agent, and an intake-form agent. Each agent has different PHI scopes. Each is invoked in different contexts. Each may be running on a different model.
The chain-of-custody problem. When five agents coordinate on the same patient encounter, whose credential authenticated the workflow? Whose authorization triggered the write? Whose accountability applies if something goes wrong? The answer in a HIPAA compliant system is that every agent is bound to the human authorizer who initiated the parent workflow, and every log entry carries both the agent identity and the delegating human identity. This is a data model decision made at platform-design time; it cannot be bolted on.
The maker-checker pattern as a HIPAA-native primitive. Maker-checker means the AI proposes an action, a human confirms, and the server re-checks the action against policy before executing it. In agentic AI, this pattern doubles as a compliance control. The maker action is the agent's proposal, captured in the audit trail with its full reasoning. The checker action is the human confirmation, captured with the confirming user's identity and timestamp. The server re-check is the ABAC evaluation before the write commits. This structure gives an auditor everything they need to reconstruct the decision after the fact — reasoning, human oversight, and policy enforcement all in one immutable record.
Human-in-the-loop as a compliance control, not a UX pattern. The HIPAA Security Rule does not require human review of every AI action. It requires that access to PHI be governed, minimum-necessary, and auditable. Human-in-the-loop becomes a compliance control when you use it strategically — for actions that materially affect care, actions that touch high-sensitivity PHI categories (behavioral health, HIV status, substance use disorder records under 42 CFR Part 2), or actions where the model's confidence is below a defined threshold. Reserve human review for where it adds compliance value; automate the low-risk actions the audit trail alone can defend.
Deployment Patterns: On-Premise, VPC-Isolated, BYOK, and Model-Agnostic Routing
Where and how you deploy a HIPAA compliant agentic AI system matters as much as how you architect it.
On-premise deployment puts the entire platform — inference gateway, agent runtime, semantic layer, audit logs — inside the covered entity's own data center. Highest control, highest operational cost, appropriate for the most sensitive workloads (behavioral health integration, research datasets under IRB restriction, systems handling substance use disorder records). Every packet stays inside the physical perimeter.
VPC-isolated cloud deployment places the platform inside a single-tenant Virtual Private Cloud in the covered entity's cloud account, with no shared inference infrastructure and no shared vector store. This is the sweet spot for most enterprise healthcare deployments — cloud scalability with a hard tenant boundary. All BAAs are direct between the covered entity and each cloud service, with the platform vendor as a business associate for the platform layer only.
Multi-tenant SaaS is structurally the wrong pattern for high-sensitivity clinical workloads. Even with strong logical isolation, a shared inference infrastructure means a leak in one tenant's sanitization pipeline can expose another tenant's payloads to the model provider. It is possible to run some non-clinical healthcare workloads on multi-tenant SaaS with the right controls, but for anything touching clinical PHI at scale, isolated deployment is the answer.
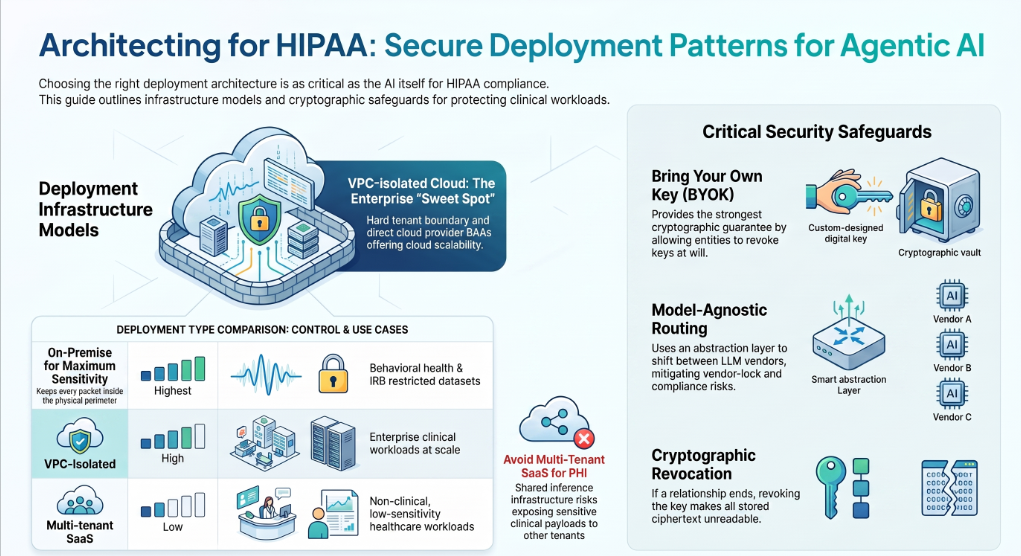
BYOK (Bring Your Own Key). Encryption keys the covered entity controls, rotated on the covered entity's schedule, revocable at will. Under BYOK, if the covered entity ever needs to terminate the relationship, they revoke the key and every ciphertext the platform ever wrote becomes unreadable. This is the strongest cryptographic guarantee available and it is a HIPAA best practice for any deployment involving highly sensitive PHI. Assistents.ai supports per-organization BYOK natively.
Model-agnostic routing. Locking the agentic AI system to a single LLM vendor is a compliance risk. If the vendor's BAA terms change, if their data-handling policies shift, if a regulatory action affects their infrastructure, the covered entity is stuck. A model-agnostic architecture routes inference through an abstraction layer — Vercel's AI Gateway, LiteLLM, or a custom router — and can shift between OpenAI, Anthropic, Google, Bedrock, or a self-hosted open-weights model without changing agent code. The Assistents platform is model-agnostic by design and supports per-organization model routing.
An End-to-End Trace: What a Governed Agent Action Actually Looks Like
Abstract architecture is helpful. A concrete trace is unforgettable. Consider a simple workflow: a scheduling coordinator at a specialty clinic asks the platform's chat interface, "Reschedule Mrs. K's follow-up from Thursday to next Tuesday afternoon."
Here is what happens under the hood in a HIPAA compliant agentic AI system.
The coordinator's authenticated session opens the request. The platform binds this workflow to the coordinator's identity and timestamps the invocation. The natural-language request goes to a router agent, which classifies the intent as a scheduling update and identifies the affected patient reference. The router agent does not have the coordinator's full RBAC — it inherits an ABAC decision scoped to scheduling actions and to the specific patient the coordinator has an active care relationship with. If the coordinator did not have that relationship, the ABAC engine denies the request at this step and the denial is logged.
The scheduling agent takes over. It queries the calendar system through a governed connector — the query is folded with a row-level predicate that scopes results to this patient only, and only to scheduling-relevant fields. The full clinical chart never appears. The agent identifies the current appointment and the requested new slot, and generates a proposed update.
Because this is a write action, maker-checker fires. The agent proposes the update, the platform presents it to the coordinator as a one-tap confirmation: "Move Mrs. K's follow-up from Thursday 2:15 PM to Tuesday 3:00 PM. Confirm?" The coordinator confirms. The server re-checks the ABAC decision, verifies the patient reference and the field-level permissions, and commits the write to the calendar system.
Every step is logged. The audit record for this single reschedule contains: the coordinator's authenticated identity, the router agent's classification result, the scheduling agent's query and reasoning, the ABAC policy decisions at each step, the model version and prompt hash used for the agent reasoning, the proposed change, the human confirmation event with timestamp, the server re-check result, and the final calendar state. If an OCR auditor asks six months later, "Show me every action taken on Mrs. K's record in Q3," the platform returns a defensible, tamper-evident sequence in seconds.
That is what "HIPAA compliant agentic AI" looks like when it works. Not a certification. Not a policy document. An architecture where every action leaves a defensible trail and every trail is the auditor's answer.
Case Studies: Governed Agentic AI in Production
Every architecture principle above is drawn from real deployments. Below are four anonymized case studies from healthcare and healthcare-adjacent environments where governed, agentic patterns are in production today.
Case Study 1 — Healthcare Staffing Platform (United States)
A workforce-matching platform connecting nursing professionals with healthcare facilities across the United States runs on a governed agentic layer. Agents handle credential capture at onboarding, facility staffing-request intake, matching logic against shift requirements, scheduling and notifications, and compliance-workflow enforcement. Every staffing decision is auditable end-to-end.
PHI-adjacent data — clinician certification data, facility identifiers, shift records — is scoped through ABAC so no agent sees fields beyond its task. Results: faster fill cycles, lower scheduling friction, improved workforce utilization, and a full HIPAA-aligned audit trail across every staffing decision. The compliance benefit is structural: the platform makes over-scoped queries impossible, so the operations team spends time on staffing outcomes, not on defending audit questions.
Case Study 2 — Physician-Led Inpatient Clinical Enterprise (New England)
A physician-led clinical enterprise operating hospitalist programs across New England deployed a governed analytics agent layer over its distributed clinical, staffing, and financial systems. Agents surface revenue-cycle leakage drivers, program-performance variance, and utilization patterns — all under RBAC that scopes analysts to their assigned programs and RLS that constrains queries to authorized data slices.
Every PHI-adjacent query is logged with the analyst's identity, the agent's SQL, and the semantic-layer policy that governed the result set. Results: improved visibility into revenue-leakage drivers, faster operational decision-making through unified reporting, and reliable performance tracking under a governance layer designed to satisfy audit expectations. The clinical enterprise moved from monthly, hand-built spreadsheets to on-demand agent-served insight without expanding its BI headcount and without expanding its compliance risk surface.
Case Study 3 — Geriatric Care Services Provider (Greater Boston)
A geriatric care services provider in the Greater Boston area delivering physician-led programs across assisted-living and long-term-care settings deployed governed agents for program-operations dashboards, staffing and service delivery analytics, and revenue-cycle exception alerts. Each user role — program operators, clinical leads, revenue-cycle managers — sees only the minimum-necessary data slices required for their function.
Row-level security is enforced at the semantic-layer query engine, so an agent answering a program operator's question about staffing utilization cannot inadvertently return billing data. Results: faster identification of operational bottlenecks, improved transparency into service performance, and better decision support for leadership across the assisted-living and long-term-care portfolio. The provider's compliance officer has an evidence pack on hand at any time; the audit conversation is now a report, not an investigation.
Case Study 4 — UK Private Healthcare and Testing Provider
A UK private healthcare and testing provider with high-volume consumer workflows deployed platform automation for testing and health-service workflows — booking through processing through reporting — with a governed operational-analytics layer on top. While the primary regulatory frame is UK GDPR and the NHS Data Security and Protection Toolkit rather than HIPAA, the architectural pattern is identical: ABAC on every access, sanitization on every model call, and immutable audit trails on every action.
The provider serves consumer-scale volumes with reduced manual overhead, fewer missed handoffs across the booking-to-reporting chain, and unified service reporting for leadership. The design lesson generalizes across regulatory frames — the four pillars work whether you are under HIPAA, GDPR, PHIPA, or PIPEDA.
Why Assistents by Ampcome
Assistents by Ampcome — spelled with an "e," a deliberate reference to the platform's enterprise-first design DNA — is a governed enterprise AI platform built by Ampcome to be the production embodiment of the reference architecture described above. Four things make it a fit for healthcare organizations building HIPAA compliant agentic AI systems.
Governance is the moat, not an add-on. The semantic layer is central to the product, not bolted onto a chat interface. Every metric definition, every access policy, every entity hierarchy lives in one place, and every agent — chat, workflow, voice — reads from that source of truth. Text-to-SQL runs over this semantic layer, which is why the platform's headline promise is "no hallucinated numbers." When a hospitalist program asks an agent for "average length of stay for cardiology admissions this quarter," the answer comes from the semantic layer's definition, folded with the row-level predicate for the asking user, executed on the customer's own warehouse — not synthesized by the model.
Maker-checker and human-in-the-loop are native primitives. Every governed write action in the platform runs through a maker-checker cycle by default. The agent proposes, a human confirms, the server re-checks the ABAC decision against the policy engine, and only then does the write commit. Human-in-the-loop is a policy configuration, not a workflow rebuild — you can require it on a per-action, per-role, per-workflow basis and change the policy without touching agent code.
Deployment topology matches HIPAA expectations. Assistents supports on-premise and VPC-isolated cloud deployments, per-organization BYOK for encryption keys, and BAA execution as part of standard enterprise onboarding. Model routing goes through Vercel's AI SDK and AI Gateway, so the platform is model-agnostic — OpenAI, Anthropic, Google Vertex, AWS Bedrock, and self-hosted open-weights models are all supported, and per-organization routing means a covered entity can pin traffic to only those model vendors it has BAAs with.
Multi-agent orchestration governed by a unified policy engine. Whether the agent is answering a clinician's question, drafting a workflow action, or handling a voice call through the telephony agent, the same semantic layer, the same ABAC policies, and the same audit pipeline apply. This is the fourth pillar — the semantic governance layer — as a shipping product surface. It is what turns a collection of agents into a compliant system.
Every case study above is a production deployment, not a pilot. If you are architecting a HIPAA compliant agentic AI system for your healthcare organization, we can help you design and deploy it.
Schedule a HIPAA architecture review at assistents.ai.
For the buyer-side complement to this architecture piece — vendor evaluation checklists, BAA negotiation guidance, and enterprise deployment framework — see our companion piece: HIPAA-Compliant AI Agents: The Complete Enterprise Deployment Guide (2026).
Check out https://assistents.ai/blogs/hipaa-compliant-ai-chatbot-2026
Common Mistakes When Architecting a HIPAA Compliant Agentic AI System
Teams building HIPAA compliant agentic AI systems tend to repeat the same mistakes. The pattern is consistent enough that any one of these is a signal that the architecture needs a review.
Assuming a signed BAA equals compliance. A BAA is a contractual promise. Compliance is an architectural fact. A vendor can sign every agreement you ask for and still be deployed in a way that violates the Security Rule. The BAA protects you legally; the architecture protects you practically.
Sharing service-account credentials across agents. This destroys chain of custody at the exact layer where the 2025 amendments expect it. Every agent needs its own identity, and every action needs to carry both the agent identity and the delegating human identity in the audit log.
Logging prompts and completions to non-BAA observability platforms. If your APM tool captures LLM inputs and outputs, and PHI ever appears in those payloads, you have just made your APM vendor a business associate — whether they signed a BAA or not. Route agent telemetry to BAA-covered observability, and sanitize before you log.
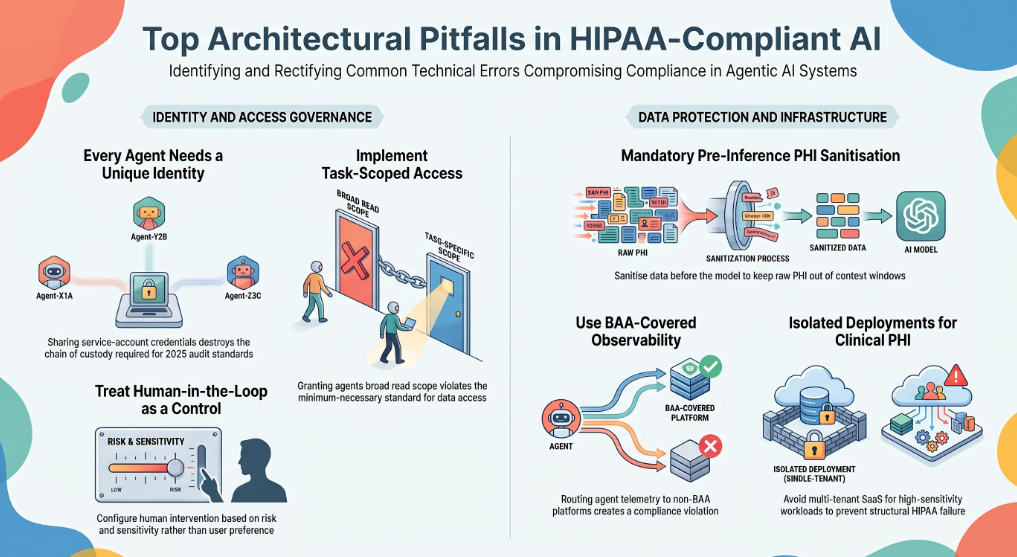
Over-scoping agent data access. The most common technical error is granting an agent broad read scope "because it might need it," rather than task-scoped ABAC. This fails the minimum-necessary standard on inspection.
Skipping pre-inference PHI sanitization because "the LLM vendor has a BAA." Defense in depth is not optional. Sanitize before the model, re-hydrate after. Even the most compliant model vendor can experience an incident, and your architecture needs to keep raw PHI out of the model's context window regardless.
Treating human-in-the-loop as a UX feature. HITL is a compliance control. Configure it against risk and sensitivity, not against user preference. Log every HITL event as part of the audit trail.
Failing to update the HIPAA risk analysis when new agents are deployed. Under the 2025 amendments, a risk analysis that predates a new AI deployment is itself an audit finding. Every material change to agent topology triggers a risk-analysis update.
Multi-tenant SaaS for high-sensitivity clinical workloads. Structural HIPAA failure regardless of how many certifications the vendor claims. For clinical PHI at scale, isolated deployment is the answer.
FAQ
Is agentic AI HIPAA compliant?
Agentic AI can be HIPAA compliant, but compliance is not a property of the AI technology — it is a property of the architecture, the vendor agreements, and the deployment. A HIPAA compliant agentic AI system enforces Attribute-Based Access Control, PHI sanitization before inference, immutable audit trails, and a unified governance layer across every agent action, and every vendor whose infrastructure touches PHI has a signed BAA with the covered entity.
Can AI agents be HIPAA compliant?
Yes, if they are deployed inside a HIPAA compliant architecture. The agent by itself is not compliant or non-compliant — it is the combination of the agent, the access controls that govern its actions, the sanitization pipeline that protects PHI in flight, the audit trail that records every action, and the BAAs with every downstream vendor that determines compliance.
What makes an agentic AI system HIPAA compliant?
Four architectural pillars: Attribute-Based Access Control for granular, context-aware PHI governance; a hybrid PHI sanitization pipeline that redacts identifiers before inference and re-hydrates them after; immutable, tamper-evident audit trails for every agent action; and a semantic governance layer that unifies policy across every agent, workflow, and downstream system. Underneath these pillars, six operational non-negotiables must hold: BAAs with every vendor, FIPS 140-3 encryption, minimum-necessary access, immutable audit, isolated deployment topology, and automated breach detection.
Is ChatGPT HIPAA compliant?
Consumer ChatGPT is not HIPAA compliant. OpenAI offers ChatGPT Enterprise and API deployments under a Business Associate Agreement for qualifying customers, with zero data retention and enterprise-grade controls, but even those must be deployed inside a broader HIPAA compliant architecture — with sanitization, ABAC, and audit — to satisfy the Security Rule. Pasting PHI into consumer ChatGPT is a HIPAA violation.
Is Claude HIPAA compliant?
Anthropic offers a Business Associate Agreement for qualifying enterprise API customers of Claude, with zero data retention and appropriate controls. Consumer Claude is not covered. As with any model vendor, a BAA with Anthropic is necessary but not sufficient — the full agentic AI system must be architected with sanitization, access controls, and audit trails to meet HIPAA requirements.
Is Microsoft Copilot HIPAA compliant?
Microsoft offers Copilot deployments under a Business Associate Agreement through Microsoft 365 Enterprise agreements, and Azure OpenAI Service supports HIPAA-compliant deployment patterns. As with all model vendors, the BAA is one component. The full architecture — how Copilot is integrated, what PHI it can access, how actions are logged — determines the overall compliance posture.
What is ABAC and why does it matter for HIPAA?
Attribute-Based Access Control is a dynamic authorization model that evaluates access decisions against attributes of the subject, resource, action, and environment in real time — rather than static role assignments alone. It matters for HIPAA because the Privacy Rule's minimum-necessary standard requires that access be limited to what a specific task requires. Static roles almost always over-scope agent access; ABAC evaluates each request against the specific task context and enforces the minimum-necessary principle structurally.
What is a PHI sanitization pipeline?
A PHI sanitization pipeline is an inference-time redaction system that removes protected health information from payloads before they reach a large language model, then re-hydrates the response inside a secure workspace so the final output is complete and clinically useful. Hybrid pipelines combine deterministic regex patterns for structured identifiers (SSNs, MRNs, dates) with a fine-tuned NER model for unstructured contextual PHI (patient names, provider names). This maps to HIPAA's Safe Harbor de-identification approach under §164.514(b)(2).
What are the 2025 HIPAA Security Rule amendments and what do they mean for AI agents?
The 2025 amendments tighten several requirements that directly affect AI agent deployments: mandatory FIPS 140-3 validated encryption for all PHI data paths, expanded direct Business Associate accountability reaching every vendor whose infrastructure touches PHI even transiently during inference, an updated risk-analysis requirement that must inventory every AI system with PHI access, and stricter expectations for chain-of-custody logging that break the "shared service account" pattern many AI deployments still rely on.
Do AI vendors need to sign a BAA?
Yes. Any vendor whose infrastructure creates, receives, maintains, or transmits PHI on behalf of a covered entity qualifies as a Business Associate under 45 CFR 160.103 and must sign a BAA before touching PHI. This includes the model host, the API gateway, the vector database, any observability platform that captures agent inputs or outputs, and any downstream integration. Under the 2025 amendments, this accountability is independently enforceable against each business associate.
What is the difference between agentic AI and generative AI under HIPAA?
Generative AI reads and generates — the compliance surface is limited to reading PHI, sending it to a model, and returning generated text. Agentic AI reads, reasons, and acts — an agent can call tools, invoke APIs, update systems of record, and coordinate with other agents. The moment an agent can create, modify, or transmit PHI on behalf of a covered entity, the compliance surface expands to cover every one of those actions. Agentic AI requires everything generative AI requires plus governed action registries, maker-checker approvals, chain-of-custody logging, and multi-agent orchestration controls.
How do you audit a multi-agent AI system under HIPAA?
Multi-agent audit requires that every log entry carry both the agent identity and the delegating human identity, that all agents in a workflow share a correlating trace ID so the sequence is reconstructable, that every action include the ABAC policy decision that governed it and the reasoning that drove it, and that logs are immutable, tamper-evident, and exported to a SIEM the covered entity controls. An auditor asking "show me every action any agent took on this patient's record" should receive a defensible sequence in seconds.
What is Assistents by Ampcome?
Assistents by Ampcome (spelled with an "e") is a governed enterprise AI platform designed around the reference architecture described in this guide — a semantic layer at the core, row-level security enforced at the data layer, maker-checker approvals native to every write action, immutable audit trails on every workflow, and BAA-ready deployment topologies including on-premise, VPC-isolated cloud, BYOK, and model-agnostic routing. It is built by Ampcome for enterprise healthcare and healthcare-adjacent organizations that need agentic AI in production without compromising HIPAA posture.

Transform Your Business With Agentic Automation
Agentic automation is the rising star posied to overtake RPA and bring about a new wave of intelligent automation. Explore the core concepts of agentic automation, how it works, real-life examples and strategies for a successful implementation in this ebook.
Sarfraz Nawaz is the CEO and founder of Ampcome, which is at the forefront of Artificial Intelligence (AI) Development. Nawaz's passion for technology is matched by his commitment to creating solutions that drive real-world results. Under his leadership, Ampcome's team of talented engineers and developers craft innovative IT solutions that empower businesses to thrive in the ever-evolving technological landscape.Ampcome's success is a testament to Nawaz's dedication to excellence and his unwavering belief in the transformative power of technology.
More insights
Discover the latest trends, best practices, and expert opinions that can reshape your perspective


.jpg)




Contact us

