

HIPAA-Compliant AI Agents: The Complete Enterprise Deployment Guide (2026)




A single OCR audit can cost a healthcare organization up to $1.5 million per violation category per year. Clinical penalties for improper PHI handling can follow for years afterward. And yet, in 2026, nearly 90% of healthcare leaders identify AI as critical to operational efficiency — while most AI adoption still stalls at the pilot stage because organizations can't answer one foundational question: Is this AI agent actually HIPAA-compliant?
A HIPAA-compliant AI agent is an autonomous AI system specifically architected to handle Protected Health Information (PHI) in accordance with the HIPAA Privacy Rule, Security Rule, and Breach Notification Rule. It isn't enough for a platform to claim compliance — the architecture, data handling, deployment model, and legal agreements must all align with federal standards before a single patient record is touched.
This guide covers everything healthcare enterprises need to know to deploy HIPAA-compliant AI agents safely: the six non-negotiables of compliant architecture, where AI agents deliver the highest ROI in healthcare workflows, what a real compliance deployment looks like, and a vendor evaluation checklist you can use immediately.
What Makes an AI Agent HIPAA-Compliant? The 6 Non-Negotiables

Not all AI platforms are built the same.
Most general-purpose AI tools are optimized for speed and scale — not the regulatory constraints healthcare demands. Before evaluating any AI agent platform, confirm that all six of the following requirements are met in full.
1. Business Associate Agreement (BAA)
The moment an AI agent processes a conversation or workflow that contains PHI, the vendor becomes a Business Associate under HIPAA. That triggers a legal requirement: a signed Business Associate Agreement (BAA) must be in place before any PHI flows through the system.
A BAA is not a courtesy document. It legally obligates the vendor to protect PHI with appropriate safeguards, to notify you of breaches within 60 days, and to accept liability for any non-compliance on their end. Without it, using an AI agent in a workflow that touches patient data is itself a HIPAA violation — regardless of how well the underlying technology is built.
Critical question to ask every vendor: Is the BAA included as a standard part of your enterprise agreement, or does it require a premium tier or custom negotiation?
2. PHI Encryption — AES-256 at Rest, TLS 1.3 in Transit
All Protected Health Information must be encrypted at rest using AES-256 encryption and in transit using TLS 1.3 (or at minimum TLS 1.2). This is a baseline, non-negotiable requirement under the HIPAA Security Rule's Technical Safeguard provisions.
What this means in practice: PHI cannot transit unencrypted across networks, cannot be stored in plaintext in logs or databases, and cannot be exposed through monitoring tooling, error messages, or debug outputs. Enterprise AI platforms that route data through shared infrastructure without encryption at every layer are fundamentally non-compliant.
3. Role-Based Access Control and the Minimum Necessary Standard
HIPAA's "Minimum Necessary" rule (§164.308(a)(3)) requires that access to PHI be limited strictly to what is required for a given task. An AI scheduling agent should be able to see calendar availability and appointment type — not a patient's clinical diagnosis or billing history.
Compliant AI agent platforms enforce granular Role-Based Access Control (RBAC) at the API layer — not just the UI layer. Each agent should be configured to access only the specific data fields required for its function, with access rules enforced automatically, not manually, at every interaction.
4. Immutable Audit Trails (§164.312(b))
HIPAA Security Rule §164.312(b) mandates that covered entities implement audit controls — hardware, software, and procedural mechanisms that record and examine activity in systems that contain or use ePHI.
For agentic AI systems, this requirement is significantly more complex than for static software. Every agent action must be logged with: the user who initiated the workflow, which data fields were accessed and when, what decision the agent made and the rationale behind it, the approval chain for any multi-step process, and a timestamp for each event.
These logs must be encrypted at rest, tamper-proof (immutable), and exportable for compliance review or OCR audit. A log that can be deleted or modified after the fact is not a compliant audit trail.
5. On-Premise or VPC-Isolated Deployment
Standard cloud AI platforms operate on shared infrastructure — your data and another organization's data may run on the same underlying compute layer. For healthcare, that multi-tenancy model is a structural compliance risk.
HIPAA-compliant AI deployments require either on-premise deployment (running entirely behind your firewall) or VPC-isolated deployment (dedicated cloud infrastructure with no shared tenancy). Under either model, PHI never leaves your environment, audit logs remain under your control, and there is no mechanism for data to bleed across customer instances.
Data residency requirements — particularly relevant for organizations operating across state lines or internationally — add another layer: the physical location of data storage must be explicitly configured and contractually guaranteed.
6. Breach Detection and Automated Notification Workflows
HIPAA requires breach notification to affected individuals within 60 days of discovery (and to HHS and media for breaches affecting 500+ individuals). For AI-driven workflows, this window is only achievable if detection is automated.
Compliant platforms implement real-time alerting on anomalous data access patterns — for example, an agent accessing a data volume far above its baseline, or accessing PHI fields outside its defined scope. These anomaly detection systems trigger compliance logs that enable rapid breach investigation and feed directly into notification workflows without requiring manual discovery.
Why Standard AI Platforms Fail Healthcare — And What to Look For Instead

Most commercial AI platforms weren't designed for healthcare. Their compliance gaps aren't marketing oversights — they're architectural decisions that made sense for their primary use cases but create real risk in regulated environments.
The PHI Exposure Risk in Shared-Tenancy Models
General-purpose Large Language Models learn from the data they process. Even with contractual data-use restrictions, a model running on shared infrastructure with shared weights creates a surface area for PHI exposure that is structurally incompatible with HIPAA. The only compliant solution is a deployment architecture where your data and model instances are fully isolated from other tenants.
The "Shadow AI" Problem in Healthcare Operations
As AI tools proliferate, healthcare staff increasingly use non-approved AI platforms to handle workloads — uploading clinical notes to consumer AI tools, running patient data through browser-based chatbots, or using unapproved summarization tools for billing documentation. This "shadow AI" behavior creates PHI exposure outside the organization's BAA coverage, outside its audit trail, and outside its breach detection systems.
Enterprise AI agent platforms address this by providing governed, approved channels for every AI-assisted workflow — channels that staff will actually use because they're fast, capable, and integrated into existing systems.
Hallucination as a Compliance Risk, Not Just a Quality Risk
In a content marketing context, AI hallucination is a quality problem. In healthcare, it's a compliance and patient safety risk. An AI agent that fabricates a diagnosis code, invents a prior authorization result, or generates an inaccurate medication instruction can expose the organization to liability that extends far beyond an OCR audit.
Compliant AI agent architectures address hallucination through retrieval-based grounding (agents work from verified data sources, not from model memory), human-in-the-loop validation gates for high-stakes decisions, and explainability logging that documents the source of every agent output.
Healthcare Use Cases Where HIPAA-Compliant AI Agents Deliver the Highest ROI
The highest-value AI agent deployments in healthcare aren't replacing clinical judgment. They're eliminating the administrative bottlenecks that consume clinician time, delay patient access, and bleed revenue. Here are the five workflow categories where HIPAA-compliant AI agents are delivering measurable results.
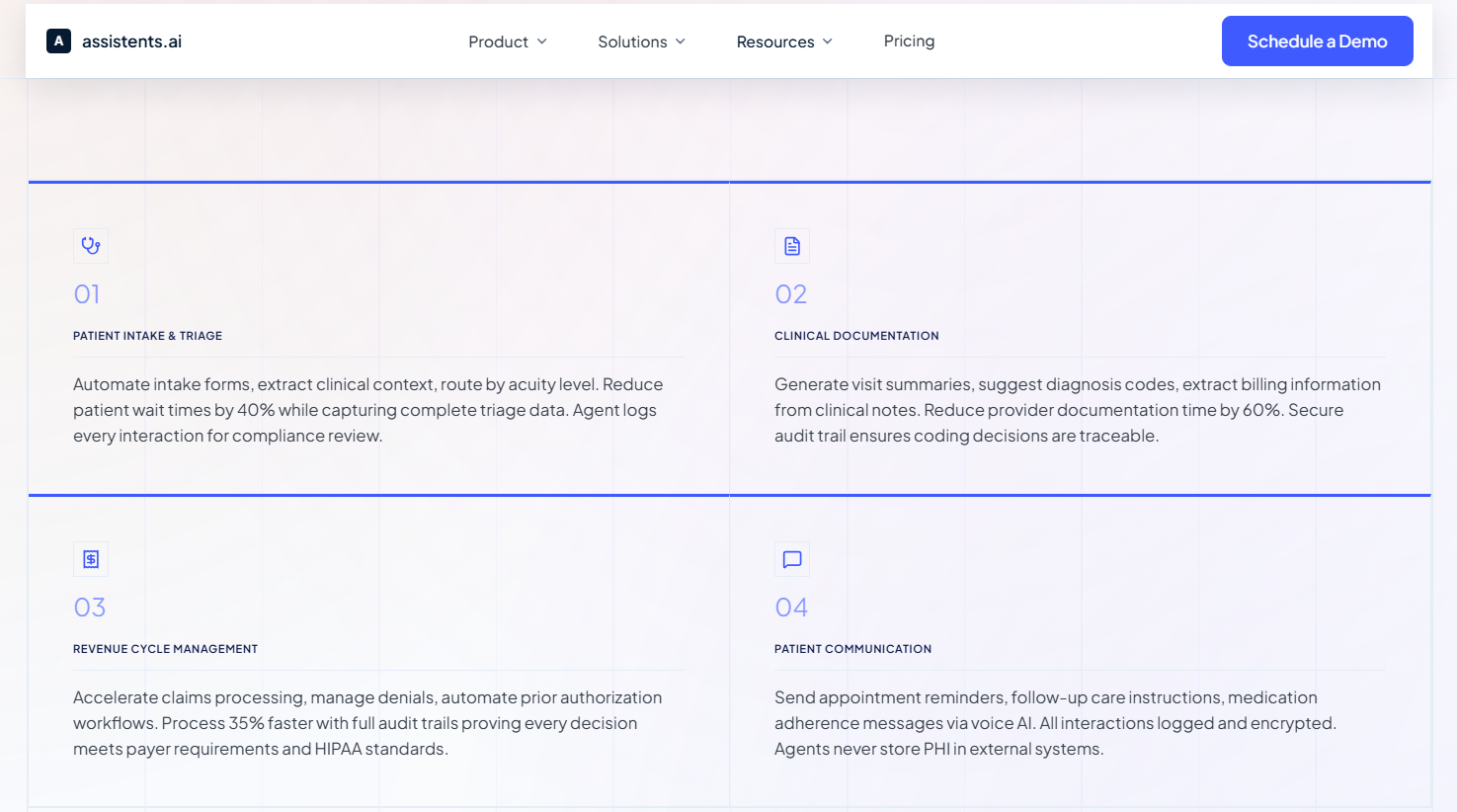
Healthcare Staffing and Scheduling Compliance Workflows
Healthcare staffing operations are operationally complex and compliance-sensitive by nature: credential verification, shift matching, facility-specific compliance requirements, and scheduling across multiple care settings all involve PHI and require auditable decisions.
AI agents in this space handle talent onboarding and credential capture, facility staffing request intake and matching logic, scheduling with automated notifications, and compliance workflow tracking for fill-rate and utilization reporting. The result is faster fill cycles, lower scheduling friction, and improved staffing responsiveness for facilities — without creating new PHI exposure surfaces.
A healthcare staffing platform operating a workforce matching model across nursing professionals and healthcare facilities deployed AI agents covering the complete staffing cycle: intake, matching, scheduling, and compliance documentation. The deployment improved fill cycles measurably, reduced the manual coordination burden on operations staff, and maintained a complete audit trail across every staffing decision — meeting HIPAA requirements without adding compliance overhead.
Inpatient Program Operations and Revenue Analytics
Physician-led inpatient enterprises face a specific operational challenge: the data required to manage program performance — census, utilization, billing outcomes, denial trends — is distributed across systems that don't talk to each other, each containing PHI that requires governed access.
AI agents in this context act as a governed analytics layer: ingesting data from multiple clinical and financial systems, surfacing revenue and utilization analytics, generating performance dashboards with variance explanations, and creating action lists for billing workflow optimization — all within a HIPAA-compliant data architecture with RBAC and full audit trails.
A physician-led clinical enterprise with inpatient programs across multiple facilities deployed AI agents for revenue management and operational performance optimization. The platform delivered improved visibility into revenue leakage drivers, faster operational decision-making through unified reporting, and more reliable performance tracking — with every data access governed and logged for compliance readiness.
Geriatric Care Service Delivery and Performance Monitoring
Geriatric care providers operate at the intersection of complex patient populations, multi-payer reimbursement environments, and strict regulatory requirements around care quality reporting. Program performance data is critical to operational decisions but is often locked in siloed systems with inconsistent definitions.
AI agents in geriatric care settings handle program operations dashboards, staffing and service delivery analytics, and revenue cycle visibility with exception alerts — surfacing the right information to the right stakeholder with the right level of PHI access, governed at every layer.
A geriatric care services provider delivering physician-led programs across assisted living and long-term care settings deployed AI agents to improve operational transparency and decision support. Results included faster identification of operational bottlenecks, improved transparency into service performance, and better decision support for leadership — all within a HIPAA-compliant architecture that maintained audit trails across program operations and financial workflows.
Patient Communication and Care-Program Support at Scale
Appointment reminders, follow-up care instructions, medication adherence messages, and care navigation support represent enormous volumes of patient communication — all of which involve PHI and all of which are traditionally handled by staff who are increasingly stretched thin.
HIPAA-compliant AI voice agents and conversational agents handle this communication layer at scale: PHI never stored in external systems, all interactions logged and encrypted, human escalation paths clearly defined, and the agent's scope restricted to the minimum necessary data for each interaction type.
Compliant patient communication agents reduce no-show rates through proactive outreach, improve care adherence through timely follow-up, and free clinical staff to focus on interactions that require human judgment — while maintaining a complete, auditable record of every patient touchpoint.
Revenue Cycle Management with Full Audit Trails
Revenue cycle workflows — claims processing, prior authorization, denial management, billing code validation — are among the most complex, PHI-intensive processes in healthcare. They're also where AI delivers some of the fastest measurable ROI, because the manual effort involved is high and the cost of errors (denied claims, delayed reimbursement, audit exposure) is significant.
AI agents in RCM workflows automate claims review and coding validation, identify missing diagnosis codes and flag them for provider review, manage prior authorization initiation and follow-up, and generate audit trails that prove every decision was justified.
An example audit trail for a single claims processing event captures: which user initiated the workflow, which claim was accessed and when, what data fields the agent read, the rule that triggered any flag, the recommended code and rationale, and approval by a billing manager — a complete chain that satisfies OCR audit requirements.
HIPAA AI Agent Architecture: What a Compliant Deployment Actually Looks Like

Understanding the compliance requirements is one thing. Understanding what a compliant AI deployment actually looks like in practice — the infrastructure decisions, the governance layer, the agent configuration — is what enables healthcare organizations to move from evaluation to production.
On-Premise vs. VPC-Isolated vs. Multi-Tenant: Why the Choice Matters for PHI
Three deployment models exist for enterprise AI agents. Only two of them are HIPAA-appropriate.
On-premise deployment runs entirely behind the organization's own firewall. The AI agent infrastructure — compute, storage, model weights, and logs — lives within the organization's own network perimeter. This is the highest level of data control and is often preferred by organizations with existing data center infrastructure or particularly sensitive patient populations.
VPC-isolated deployment gives the organization dedicated cloud infrastructure with no multi-tenancy. The organization's agents, data, and logs run in a logically and physically isolated environment within a cloud provider's infrastructure. PHI never shares compute resources with another customer's data. This model provides the scalability of cloud with the isolation requirements of healthcare.
Multi-tenant cloud — the standard model for most commercial AI platforms — is not appropriate for PHI. Data residency is undefined, shared compute creates structural exposure risk, and the audit trail typically doesn't meet §164.312(b) requirements.
How Audit Logs Must Work in Agentic Systems
Traditional software audit logs capture user actions. Agentic AI systems require a fundamentally more detailed log architecture because the agent itself is making decisions — decisions that must be explainable, traceable, and defensible under audit.
A compliant agentic audit log captures every event in a decision chain: the trigger (what initiated the workflow), the data accessed (which fields, at what timestamp), the reasoning (what rule or logic drove the agent's action), the output (what the agent recommended or executed), the human validation step (if applicable), and the final state (what happened as a result). These logs must be encrypted at rest, stored in an immutable format (not modifiable after creation), and exportable in a structured format for compliance review.
Governing Multiple AI Agents Simultaneously in a Healthcare Environment
Most healthcare enterprises don't deploy a single AI agent — they deploy several, covering different workflow domains (patient communication, RCM, staffing, documentation) with different data access requirements and different risk profiles. Governing this multi-agent environment requires a purpose-built governance layer.
An enterprise AI agent governance framework defines access policies at the agent level (not just the user level), implements semantic rules that govern how agents interpret and act on data, maintains a complete orchestration log across all agent activity, and provides a single administrative view for compliance officers to monitor agent behavior across the entire deployment.
Without a governance layer, each AI agent deployment becomes a separate compliance risk to manage individually — which scales poorly and creates gaps that are difficult to detect until an audit exposes them.
HIPAA Compliance Checklist for Evaluating AI Agent Vendors (2026)
Use this checklist when evaluating any AI agent platform for healthcare deployment. Every item should be confirmed in writing — in the contract, the BAA, or documented security controls — before any PHI flows through the system.
- BAA availability — Does the vendor offer a BAA as a standard part of their enterprise agreement? (Not a premium add-on, not subject to custom negotiation)
- Encryption standards — Is PHI encrypted at rest with AES-256 and in transit with TLS 1.3 or 1.2 minimum?
- Deployment isolation — Does the vendor offer on-premise or VPC-isolated deployment? Is multi-tenant architecture excluded from PHI-handling workflows?
- RBAC enforcement — Is role-based access control enforced at the API layer, not just the UI? Can agent-level data access be scoped to specific fields?
- Audit trail completeness — Does the audit log capture the full decision chain (trigger, data accessed, reasoning, output, approval)? Are logs immutable and exportable?
- Zero PHI data retention — Is PHI retained after processing? Is the vendor using customer data to train or improve their models?
- Breach detection and alerting — Does the platform include real-time anomaly detection on data access patterns? Does it feed into automated notification workflows?
- Third-party certification — Does the vendor hold SOC 2 Type II certification? Is HITRUST certification available or in progress?
- Sub-processor transparency — What third-party services does the vendor use? Do all sub-processors have their own BAAs in place?
- Data residency — Can you specify the geographic location of data storage? Is US-based hosting guaranteed for PHI workloads?
- Human-in-the-loop controls — For high-stakes decisions (clinical coding, prior auth, denial management), does the platform support mandatory human validation gates?
- Governance layer — For multi-agent deployments, does the platform provide centralized policy management and a compliance officer view across all agent activity?
Common Deployment Mistakes That Create HIPAA Risk
Even organizations that choose a compliant platform can create compliance exposure through implementation decisions. These are the most common mistakes healthcare teams make when deploying AI agents.
Assuming vendor compliance means organizational compliance. A BAA protects you legally. Proper configuration, access management, staff training, and ongoing audit review protect you practically. HIPAA compliance is a shared responsibility — the vendor provides the compliant infrastructure; your organization must use it correctly.
Skipping the sub-processor audit. An AI platform vendor may sign your BAA, but if they route data through a third-party analytics tool, a logging service, or a model inference provider that isn't covered by its own BAA, you have a compliance gap. Always request a full sub-processor list and confirm BAA coverage at every layer.
Deploying without a tabletop breach exercise. Most organizations discover gaps in their breach response runbook during an actual incident, not before it. Before go-live, run a realistic breach scenario (for example: an agent accidentally logging a prompt containing PHI to a non-BAA observability tool). Walk through detection, containment, patient notification, and HHS reporting with your privacy officer, legal counsel, and engineering lead. The 60-day notification window is unforgiving.
Not scoping agent data access before deployment. Agents configured with broad data access — even "read-only" access — create unnecessary exposure surface. Every agent should be configured with the minimum data fields required for its specific workflow before it goes into production, not as a later optimization.
Treating HIPAA compliance as a one-time setup. OCR enforcement has increased significantly between 2024 and 2026. Compliance is an ongoing process: access rights must be reviewed as staff roles change, agent configurations must be audited as workflows evolve, and audit logs must be reviewed on a regular cadence — not only when an incident occurs.
Deploy HIPAA-Compliant AI Agents With Confidence
assistents.ai is built for healthcare enterprises that cannot afford compliance gaps. Our platform meets HIPAA, HITECH, and SOC 2 Type II requirements out of the box: BAA-ready, on-premise and VPC-isolated deployment options, immutable audit trails mapped to HIPAA Security Rule requirements, and granular RBAC enforced at the API layer.
Every AI agent deployment starts with a HIPAA architecture review — a structured session where we walk through your specific workflows, data access requirements, and compliance obligations before a single line of configuration is written.
FAQs
Can AI agents be HIPAA-compliant?
Yes — when built on the right infrastructure and deployed correctly. A HIPAA-compliant AI agent requires a signed Business Associate Agreement with the vendor, PHI encryption at rest and in transit, role-based access control enforced at the API layer, immutable audit trails covering every agent decision, and an isolated deployment architecture (on-premise or VPC-isolated) that prevents PHI from sharing infrastructure with other tenants. Compliance is an architectural requirement, not a feature layer added after the fact.
What is a BAA in the context of an AI agent?
A Business Associate Agreement is a legally binding contract required by HIPAA whenever a vendor handles Protected Health Information on behalf of a covered entity. The moment an AI agent processes a workflow containing PHI — even a single data field from a patient record — the vendor becomes a Business Associate and a BAA must be in place. The BAA obligates the vendor to protect PHI with appropriate safeguards, notify you of breaches within 60 days, and accept liability for non-compliance on their end.
Is on-premise deployment required for HIPAA AI agents?
Not necessarily — VPC-isolated cloud deployment is also HIPAA-appropriate when implemented correctly. The key requirement is that PHI must not share infrastructure with other organizations' data (no multi-tenancy). On-premise deployment gives the highest level of control; VPC-isolated deployment provides equivalent isolation with cloud-scale flexibility. Standard multi-tenant cloud infrastructure is not appropriate for PHI-handling AI workflows.
What is the difference between HIPAA compliance and SOC 2 for AI platforms?
HIPAA governs the handling of Protected Health Information specifically in the US healthcare context. SOC 2 Type II is an independent audit certification that verifies a vendor's internal controls for security, availability, processing integrity, confidentiality, and privacy over a sustained period. For healthcare AI deployments, you want both: SOC 2 Type II confirms the vendor's general security posture; HIPAA BAA and compliance controls confirm they can specifically handle PHI. SOC 2 alone does not make a platform HIPAA-compliant.
Can a HIPAA-compliant AI agent handle voice workflows?
Yes. HIPAA-compliant voice AI agents operate under the same requirements as any other AI agent handling PHI: BAA in place, audio data encrypted in transit and at rest, interaction logs maintained in an immutable audit trail, PHI never stored in external systems or exposed to third-party transcription services outside BAA coverage, and human escalation paths clearly defined. Voice workflows — appointment reminders, care instructions, patient communication — are appropriate for AI agents when the underlying platform meets these requirements.
How do audit trails work for agentic AI in a HIPAA context?
Unlike traditional software, where audit logs capture user actions, agentic AI systems require logs that capture the full decision chain: what triggered the workflow, which data fields the agent accessed and when, what rule or logic drove the agent's action, what the agent recommended or executed, whether human validation occurred, and what the final outcome was. These logs must be encrypted at rest, stored in an immutable format (meaning they cannot be modified after creation), and exportable for compliance review. §164.312(b) of the HIPAA Security Rule mandates these audit controls for any system containing or using ePHI.
What happens if a HIPAA-compliant AI agent causes a PHI breach?
HIPAA's Breach Notification Rule requires notification to affected individuals within 60 days of discovery, notification to HHS (and to media for breaches affecting 500 or more individuals in a state), and documentation of the breach and response. If a BAA is in place and the vendor failed to meet their contractual obligations, liability is shared — the BAA specifies the vendor's responsibilities. If the breach resulted from the organization's own misconfiguration or improper use of an otherwise compliant platform, organizational liability is primary. This is why proper configuration, access management, and pre-deployment breach exercises are as important as vendor compliance certifications.

Transform Your Business With Agentic Automation
Agentic automation is the rising star posied to overtake RPA and bring about a new wave of intelligent automation. Explore the core concepts of agentic automation, how it works, real-life examples and strategies for a successful implementation in this ebook.
Sarfraz Nawaz is the CEO and founder of Ampcome, which is at the forefront of Artificial Intelligence (AI) Development. Nawaz's passion for technology is matched by his commitment to creating solutions that drive real-world results. Under his leadership, Ampcome's team of talented engineers and developers craft innovative IT solutions that empower businesses to thrive in the ever-evolving technological landscape.Ampcome's success is a testament to Nawaz's dedication to excellence and his unwavering belief in the transformative power of technology.
More insights
Discover the latest trends, best practices, and expert opinions that can reshape your perspective






Contact us

