

AI Agents in Cancer Research and Oncology: Use Cases, Capabilities and Deployment Guide (2026)




In late 2024, Nature Cancer published a landmark perspective declaring that AI agents will fundamentally change how cancer research and oncology work. The paper described a new generation of autonomous systems capable of planning, executing, and optimising multi-step biomedical workflows — without constant human input.
The research world took notice. The enterprise world did not know what to do with it.
Most healthcare organisations, digital health operators, and clinical research teams understand that AI agents are coming. What they lack is a clear, practical picture of what these agents actually do, where they are being deployed right now, what the real implementation challenges look like, and how to choose the infrastructure to run them safely.
This guide closes that gap.
Whether you are a healthcare CIO evaluating agentic AI platforms, a clinical informatics leader scoping a pilot, or a life sciences team looking to automate research workflows, this is the piece you will want to bookmark and share.
What Are AI Agents — and Why Are They Different from Traditional AI in Healthcare?
AI agents in cancer research and oncology are not simply smarter chatbots or upgraded diagnostic models. They represent a fundamental shift in what artificial intelligence can do inside a healthcare or research organisation.
Traditional AI in healthcare — the kind that has been in use for decades — excels at narrow, well-defined tasks: reading a mammogram, flagging an anomalous lab result, predicting a readmission risk score. These systems are powerful, but they are passive. They wait to be asked a question, produce an output, and stop. They cannot plan a sequence of actions. They cannot pick up a tool, check a live system, make a decision, and then log what they did. Every step beyond the model's single task requires a human.
AI agents are different because they can act across a sequence of steps. They sense their environment — reading documents, querying databases, ingesting live signals. They plan — breaking a complex goal into sub-tasks. They execute — taking action inside connected systems. And they learn from outcomes, adjusting their approach in subsequent runs. A single agent can do in seconds what previously required a handoff between three departments.
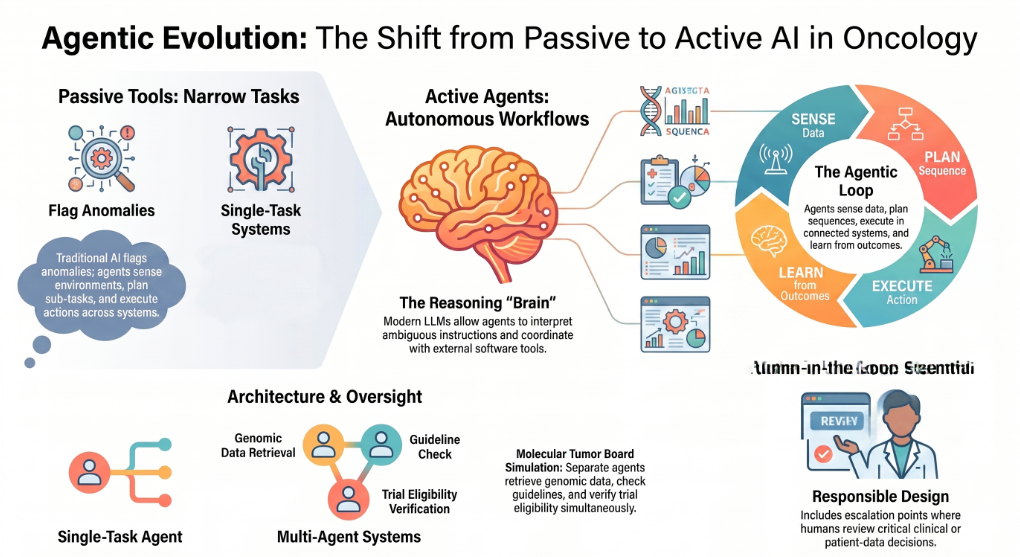
What makes this possible is the emergence of large language models (LLMs) with genuine reasoning capability. Since 2022, LLMs have moved well beyond pattern recognition and text generation. They can now orchestrate complex workflows, interpret ambiguous instructions, and coordinate with external tools and software. This is what allows an LLM to function as the brain of an agent — not just generating words, but directing action.
In cancer research and oncology specifically, two agent architectures matter most.
Single-task agents handle one discrete workflow: retrieving and summarising a body of literature, screening a compound library, flagging an anomaly in a genomic dataset. They are easier to validate, easier to govern, and the right starting point for most organisations.
Multi-agent systems are orchestrated networks of specialised agents working in sequence or in parallel. Think of a molecular tumour board simulation: one agent retrieves and synthesises the patient's genomic data, a second cross-references current clinical guidelines, a third checks trial eligibility, and a fourth drafts a treatment recommendation with citations — all before a clinician opens the file. Each agent does what it does best. The orchestrator connects them.
One concept that matters enormously in clinical settings is human-in-the-loop design. Fully autonomous agent runs — where no human reviews the output before it triggers an action — are appropriate for some administrative and operational workflows. For anything touching clinical decisions or patient data, a well-designed agent architecture always includes configurable escalation points: moments where the system flags uncertainty, pauses, and routes to a human reviewer before proceeding. This is not a limitation of the technology. It is how responsible agentic AI is built.
How AI Agents Are Being Applied in Cancer Research Today
The evidence base for AI agents in cancer research is emerging rapidly, spanning four major application areas. Each represents a genuine departure from what previous generations of AI could do.
Drug Discovery and Target Identification
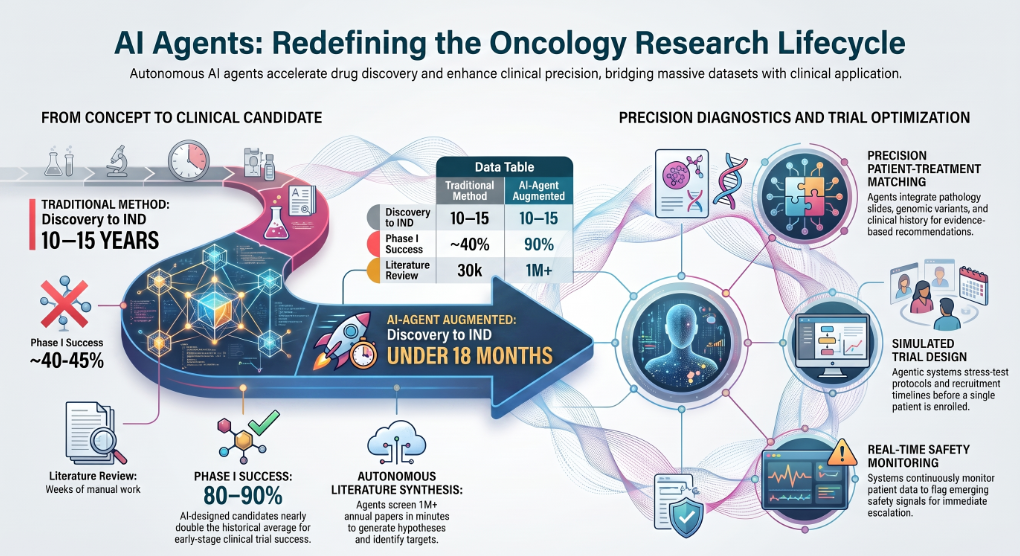
Traditional drug discovery is brutally slow. A candidate molecule typically takes ten to fifteen years to travel from initial identification to regulatory approval, with failure rates exceeding ninety percent at the clinical trial stage. The bottleneck is not scientific knowledge — it is the speed at which researchers can synthesise, test, and interpret the results of thousands of candidate compounds.
AI agents are beginning to compress that timeline in ways that were not possible even three years ago. Autonomous agents can now plan and execute complete drug discovery sub-workflows: ingesting published literature and proprietary assay data, generating molecular hypotheses, simulating compound behaviour against target proteins, ranking candidates by predicted efficacy and safety profile, and flagging the most promising leads for experimental validation — all without waiting for a human to connect each step.
The results are striking. AI-designed drug candidates are currently achieving Phase I clinical trial success rates of eighty to ninety percent, nearly double the historical average. One AI-developed compound — a small-molecule inhibitor designed autonomously by an LLM-based research agent — progressed from concept to Investigational New Drug application in under eighteen months, a timeline that would have been considered impossible through conventional means.
In oncology specifically, agents are being used to identify novel inhibitors of cancer-relevant targets, propose therapeutic strategies for specific tumour profiles, and surface candidate compounds that human researchers had not considered. The agents do not replace the scientist's judgment. They radically expand the search space the scientist can explore.
Clinical Trial Design and Recruitment
Clinical trial failure is one of the most expensive problems in medicine. More than half of oncology trials fail not because the drug does not work, but because of protocol design issues, inadequate patient stratification, or recruitment shortfalls. AI agents address all three.
Agentic systems can read and interpret complex trial protocols, cross-reference eligibility criteria against patient records written in unstructured natural language, flag likely candidates in a population, and automatically monitor enrolled patients for protocol deviations. They can also simulate trial designs before a single patient is enrolled — stress-testing inclusion criteria, modelling recruitment timelines, and identifying statistical risks in adaptive trial structures.
The operational impact goes further. Agents that continuously monitor incoming patient data during an active trial can detect emerging safety signals, flag deviations from expected response curves, and escalate to the data safety monitoring board with a structured evidence summary — tasks that currently require weeks of manual analysis.
Genomic and Pathology Analysis
Precision oncology depends on the ability to match a patient's specific tumour biology — its genomic variants, expression patterns, immune profile — to the most appropriate treatment. This matching problem is extraordinarily complex. A patient's tumour can carry hundreds of variants. The clinical evidence connecting those variants to treatment response is scattered across thousands of papers, trial reports, and databases, updated constantly.
AI agents are well-suited to this problem because it requires exactly the kind of multi-step reasoning they excel at. A multimodal agent can ingest pathology slides, genomic sequencing data, clinical history, and current guideline documents simultaneously, synthesise the relevant evidence, and produce a structured treatment recommendation with citations — surfacing the reasoning so a clinician can evaluate it, not just accept it.
Vision-language agents — models that combine image understanding with text reasoning — are demonstrating strong performance in digital pathology, interpreting slide images at a level of consistency that human pathologists find difficult to sustain across high volumes.
Literature Review and Research Automation
Every oncology researcher is losing the battle against the literature. More than one million cancer-related papers are published annually. No team can read everything relevant. Important findings are missed. Research directions are duplicated. Evidence that should inform a clinical decision sits uncited in a database.
AI research agents change this dynamic. An agent configured for systematic literature review can autonomously retrieve papers from specified sources, screen for relevance against defined criteria, extract key findings, synthesise conflicting evidence, and produce a structured summary with citations — in minutes rather than weeks.
This is not a theoretical capability. Agentic deep research tools are already deployed in life sciences teams for competitive intelligence, regulatory evidence gathering, and hypothesis generation. The workflow an analyst would previously spend three weeks completing can be completed overnight, with the agent maintaining a live knowledge base that updates as new papers are published.
AI Agents in Clinical Oncology Operations: Decision Support, Staffing, and Workflow Automation
Beyond the research lab, AI agents are transforming the operational fabric of cancer care delivery. This is the area where the gap between academic literature and real-world deployment is widest — and where the practical impact for healthcare organisations is most immediate.
Clinical Decision Support That Explains Its Reasoning
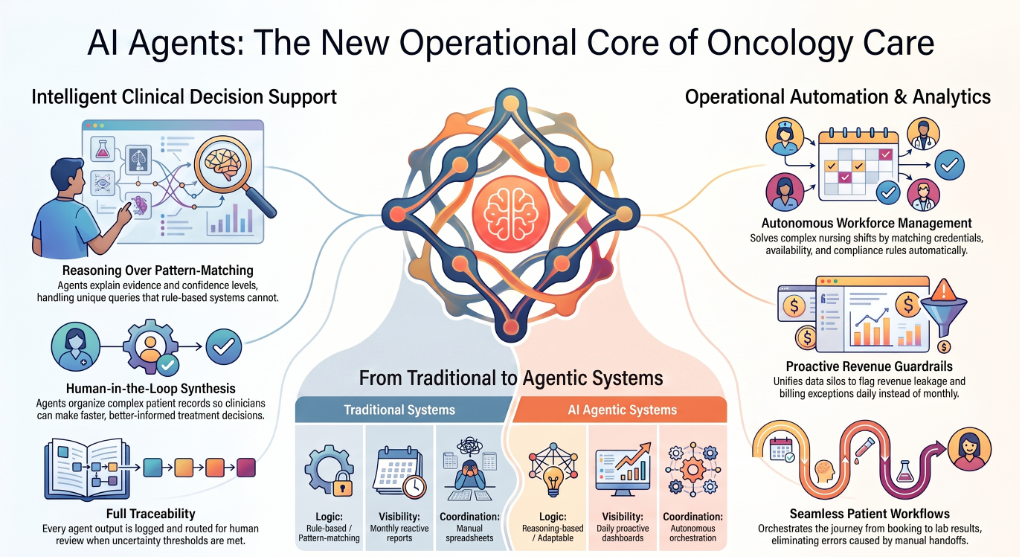
The most clinically significant deployment of AI agents in oncology is in decision support: systems that ingest a patient's full record, apply current evidence, and surface structured recommendations with the reasoning made visible.
What distinguishes agent-based decision support from older clinical decision support tools is explainability and adaptability. A traditional rule-based system tells a clinician what to do. An agent tells a clinician what it found, what evidence it applied, how confident it is, and what it did not find — and it can handle a query it has never seen before, because it reasons rather than pattern-matches.
The human-in-the-loop design principle is essential here. Clinical agents in responsible deployments are not making autonomous treatment decisions. They are doing the synthesis work — gathering, organising, and presenting evidence — so the clinician can make a faster, better-informed decision. Every agent output is logged, traceable to its source, and routable for human review when uncertainty exceeds a threshold.
Healthcare Staffing: Matching, Scheduling, and Compliance Automation
One of the most acute operational crises in oncology care delivery is workforce management. Oncology units face chronic staffing gaps. Matching credentialed nursing professionals to open shifts — accounting for specialisation, availability, compliance certifications, and facility rules — is a multi-constraint scheduling problem that hospitals currently solve through a combination of manual coordination and fragmented spreadsheets.
Agentic AI solves this problem comprehensively. In a production deployment we have been part of — a healthcare staffing platform connecting nursing professionals with healthcare facilities — an agentic system now manages the full workflow autonomously: intake of staffing requests from facilities, credential verification and matching logic, shift scheduling, automated notifications to candidates, compliance tracking, and real-time fill-rate reporting for operations leadership.
The outcomes were clear: faster fill cycles, lower scheduling friction, better workforce utilisation, and improved staffing responsiveness for facilities — all without adding headcount to the coordination function. The system escalates to a human coordinator only when a constraint cannot be resolved by the configured matching logic.
Clinical Program Operations and Revenue Analytics
Physician-led clinical enterprises — hospitalist programs, inpatient specialist groups, and post-acute care providers — operate at the intersection of clinical performance and financial sustainability. Managing that intersection well requires unified visibility across care delivery, staffing, billing, and outcomes data that typically lives in four different systems and is reported monthly at best.
In a production deployment with a physician-led inpatient clinical enterprise, an agentic analytics layer was deployed to unify data across care delivery, staffing, revenue cycle, and operational performance. The agents now produce proactive dashboards, surface revenue leakage drivers, flag billing workflow exceptions, and generate structured action lists for operational leads — daily, not monthly. The result was faster identification of operational bottlenecks, improved transparency into service performance, and better decision support for clinical leadership.
A separate deployment with a geriatric care services provider followed the same model. Agents now monitor staffing and service delivery analytics, flag anomalies in care program operations, and surface visibility into revenue cycle performance — enabling the clinical leadership team to manage financial and operational risk proactively rather than reactively.
Health Testing and Patient Workflow Automation
In high-volume consumer healthcare settings — private testing providers, diagnostic clinics, and outpatient health services — patient experience depends entirely on the reliability of the workflow connecting booking, sample processing, results reporting, and follow-up communication. Every manual handoff is a potential failure point.
In a production deployment with a private healthcare and testing provider, agentic orchestration was applied to the complete patient workflow: from booking intake through lab processing to results notification and follow-up communication. The agents manage status monitoring, trigger customer notifications at each stage, and flag exceptions for human review when a step falls outside expected parameters. The outcome was faster patient communications, fewer missed handoffs, and improved service visibility through unified reporting — with measurable reduction in the operational overhead previously required to manage these workflows manually.
The Real Challenges of Deploying AI Agents in Cancer Research and Clinical Settings
The potential of AI agents in cancer research and oncology is significant and well-evidenced. The deployment challenges are equally real, and healthcare organisations that underestimate them tend to fail at the implementation stage. Here is an honest account of where the complexity lives, and what responsible deployment looks like.
Data Privacy, HIPAA Compliance, and PHI Handling
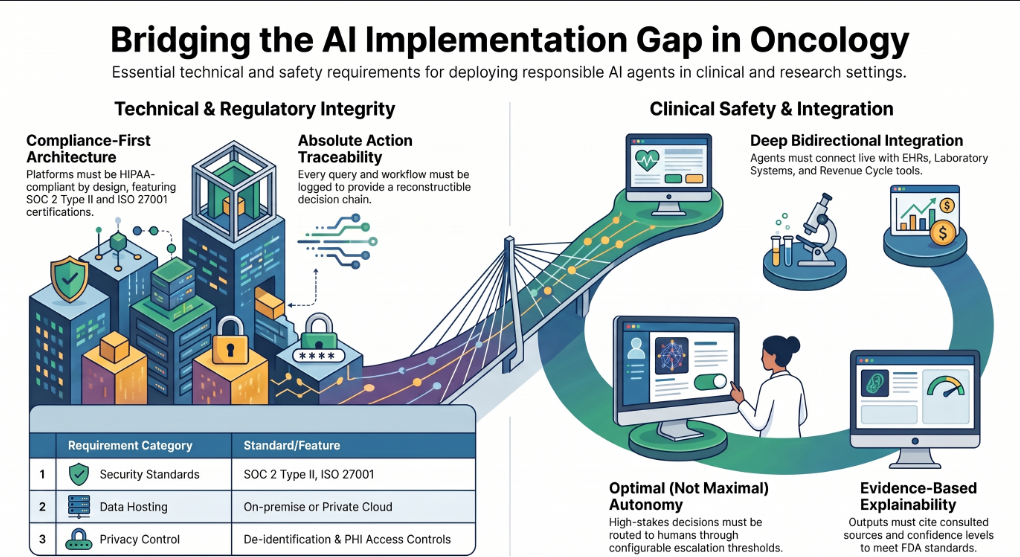
Healthcare data is the most sensitive category of personal information. Any agent that reads, processes, or acts on patient data must operate within a framework that ensures protected health information never leaves a compliant environment, every data access is logged, and the vendor infrastructure is independently audited.
This means your AI agent platform must be HIPAA-compliant by architecture — not by policy statement. Look for SOC 2 Type II certification, ISO 27001, on-premise or private cloud deployment options, and a documented approach to de-identification and PHI access controls. Platforms that were built for general enterprise use and are applying healthcare compliance as a retrofit layer are not the same as platforms designed with compliance as a foundation.
Governance: Every Agent Action Must Be Traceable
In a clinical or research environment, "the AI did it" is not an acceptable audit trail. Every action an agent takes — every query it runs, every recommendation it produces, every workflow it triggers — must be logged, attributable, and reviewable.
This requires a governance layer built into the agent platform itself: not bolted on after the fact. Rule-governed workflows define what an agent is permitted to do and under what conditions. Permission-checking ensures agents cannot access systems or data outside their defined scope. Audit logs capture the full decision chain so compliance, legal, and clinical governance teams can reconstruct exactly what happened and why.
Healthcare organisations that attempt to deploy agents without this governance infrastructure typically hit a wall at their first compliance review — or worse, after an incident.
Multi-Step Workflow Complexity and Integration Depth
Healthcare operations are multi-system environments. A clinical agent that cannot read live data from an EHR, a laboratory information system, a scheduling platform, and a revenue cycle tool is not genuinely useful — it is a demo that cannot function in the real world.
Genuine agentic deployment in healthcare requires deep, bidirectional integration with the systems that hold live operational context. This is harder to build than most vendors acknowledge. It requires a context engine that normalises data from heterogeneous sources, a semantic layer that applies consistent definitions across systems, and an integration architecture that does not require months of custom development for each new data source.
Human-in-the-Loop Design for Clinical Safety
The question of when an agent should act autonomously and when it should pause and route to a human is not a philosophical one in clinical settings. It is a patient safety question.
Well-designed clinical agents are not maximally autonomous. They are optimally autonomous — doing what they can do reliably without human review, and consistently flagging the edge cases, uncertain outputs, and high-stakes decisions for human oversight. This requires deliberate architecture: configurable escalation thresholds, clear handoff protocols, and documentation of which agent actions are within autonomous scope and which are not.
Organisations that deploy fully autonomous agents in clinical contexts without these controls are not being bold. They are being reckless.
Explainability and Regulatory Readiness
The FDA has been clear that AI systems used in clinical decision support must be explainable — not just accurate. An agent that recommends a treatment without showing its reasoning, citing its evidence, or disclosing its uncertainty is not deployable in a regulated clinical environment.
Agent outputs in oncology settings should always include the evidence chain: what sources were consulted, what criteria were applied, what the confidence level is, and what the agent did not find. This is both a regulatory requirement and a clinical trust requirement. Oncologists will not trust, and should not trust, a system that tells them what to do without explaining why.
What to Look for When Evaluating an AI Agent Platform for Healthcare
If you are evaluating AI agent platforms for a healthcare, oncology, or life sciences deployment, the checklist below will help you separate platforms that are ready for clinical environments from platforms that are not.
Compliance architecture. Does the vendor hold SOC 2 Type II, HIPAA, ISO 27001 certifications? Is on-premise or private cloud deployment available? How is PHI handled at the infrastructure level, not just in policy?
Multi-agent orchestration. Can the platform run coordinated networks of specialised agents, not just single-model workflows? Can you configure how agents communicate, how conflicts are resolved, and how handoffs between agents are logged?
Context depth. Does the platform read live operational data from the systems you already run — EHR, LIS, scheduling, billing — or does it require data to be extracted and uploaded manually? A context engine that pulls live data is fundamentally more capable than one that operates on static document stores.
Governance layer. Is every agent action rule-governed, permission-checked, and audit-logged by default? Can you define exactly what an agent is and is not permitted to do? Can a compliance team pull a complete action log for any agent run?
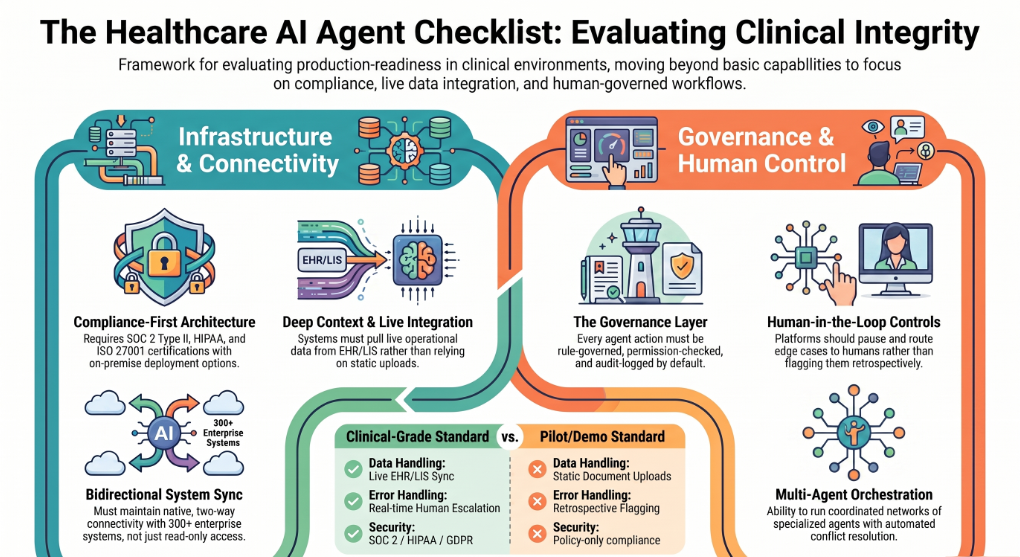
Human-in-the-loop controls. Can you configure escalation thresholds? When an agent is uncertain or encounters an edge case, does it pause and route to a human reviewer, or does it proceed and flag retrospectively? The former is the correct design for clinical environments.
Integration breadth. How many enterprise systems does the platform connect to natively? How long does a new integration take to configure? Can the platform maintain bidirectional sync with clinical systems, not just read-only access?
Proof of production deployment in healthcare. Has the vendor deployed agentic AI in live healthcare environments — not pilots, not demos — with documented outcomes? Can they speak to what governance challenges emerged and how they were resolved?
Assistents, built by Ampcome, was designed from the ground up for governed, auditable, HIPAA-compliant agentic AI deployment. It connects to over three hundred enterprise systems, runs on infrastructure you control, and carries SOC 2 Type II, HIPAA, ISO 27001, and GDPR certifications. Its Agent Governance layer ensures every action is policy-checked, permission-bounded, and logged. It is already in production across healthcare staffing, clinical program operations, patient workflow automation, and health services analytics — the deployments described in this article are drawn from that live portfolio.
What's Next: AI Agents and the Future of Cancer Research
The trajectory of AI agents in cancer research and oncology is steep, and the near-term developments are already visible.
Clinical trials as the new frontier. The major pharmaceutical companies have shifted their AI investment focus. Drug discovery attracted the first wave of attention and capital. Clinical trials — historically the last untouched bottleneck — are now the primary target. Discovery cycles that previously took years are being compressed to months. Autonomous agentic systems that bridge the wet lab and the computational dry lab, running continuously, are beginning to close the loop between hypothesis, experiment, and clinical validation.
AI-driven biomarkers embedded in clinical workflows. Biomarker identification — the ability to predict which patients will respond to which therapies — has historically required expensive, specialised assays. Emerging agentic models trained on routine labs, imaging, and genomic data are beginning to identify predictive biomarkers from data that already exists in hospital records, without requiring additional testing. The near-term prospect is biomarker intelligence embedded directly into clinical workflows, surfacing treatment guidance at the point of care.
Multi-agent tumour boards. The molecular tumour board — a multidisciplinary clinical team reviewing a patient's tumour biology to plan treatment — is one of oncology's most resource-intensive and access-constrained processes. Specialist oncologists are scarce and concentrated in major academic centres. Multi-agent AI systems are beginning to simulate the tumour board process: multiple specialised agents collaborating — genomics agent, pathology agent, guidelines agent, trial eligibility agent — to produce a structured, evidence-backed treatment plan that a clinician then reviews and acts on. This will not replace the tumour board. It will make the tumour board's level of analysis accessible to the patient who cannot get to a major cancer centre.
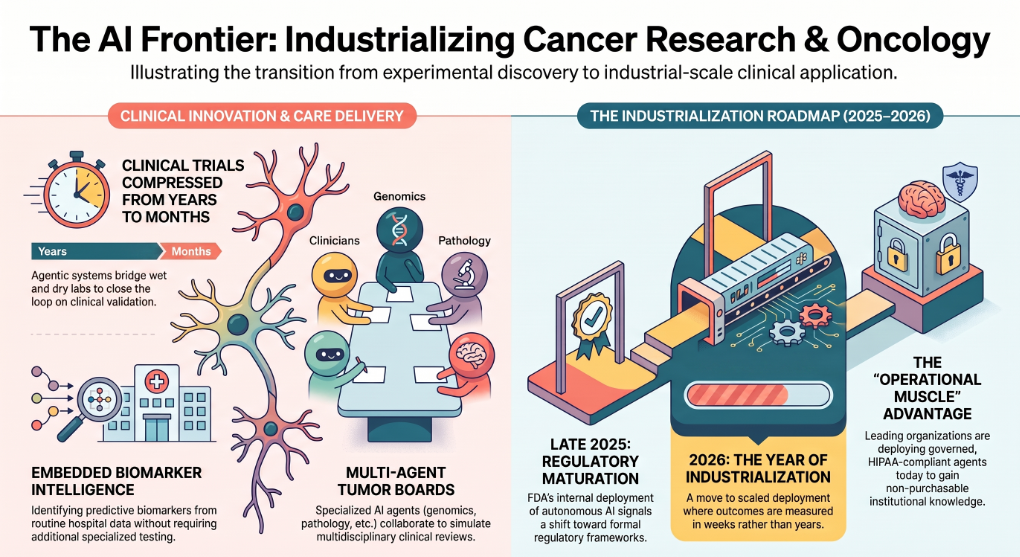
Regulatory maturation. The FDA's deployment of autonomous AI for internal administrative workflows in late 2025 signalled that regulatory bodies are moving from observation to adoption. The frameworks governing AI agents in clinical settings are developing, but healthcare organisations that build on compliant, auditable infrastructure today will be positioned to operate within those frameworks as they formalise — rather than having to retrofit compliance into systems that were not designed for it.
The year of industrialisation. 2026 has been called the year of AI industrialisation in oncology by leading voices at the JP Morgan Healthcare Conference and across the clinical AI community. The shift is from infrastructure investment to scaled, production deployment — health and pharmaceutical organisations training foundational models on proprietary data, deploying agents across entire care pathways, and measuring outcomes in weeks rather than years.
The organisations that will lead this transition are not the ones waiting for the technology to mature. They are the ones deploying governed, auditable, HIPAA-compliant AI agents in production today — learning what works, building the operational muscle, and accumulating the institutional knowledge that cannot be bought later.
Ready to Deploy AI Agents in Your Healthcare or Research Operations?
The gap between the promise of AI agents in cancer research and oncology and real operational deployment is closing fast. The organisations that will lead this transition are not waiting. They are deploying now — learning what works, building governance infrastructure, and accumulating the institutional knowledge that cannot be purchased retroactively.
Assistents is the enterprise agentic AI platform built for governed, auditable, HIPAA-compliant deployment. It runs on infrastructure you control, connects to over three hundred enterprise systems, and is already in production across healthcare staffing, clinical analytics, patient workflow automation, and health services operations.
If you are ready to move from evaluation to deployment, request a demo at assistents.ai.
Frequently Asked Questions
What are AI agents in cancer research and oncology?
AI agents in cancer research and oncology are autonomous or semi-autonomous systems powered by large language models that can plan, execute, and optimise multi-step workflows — from drug discovery and genomic analysis to clinical decision support and healthcare operations. Unlike traditional AI, which handles single tasks in isolation, agents act across sequences of steps, interact with external systems, and produce auditable outputs.
What is the difference between AI and AI agents in healthcare?
Traditional AI in healthcare performs narrow, predefined tasks: classifying an image, predicting a risk score, retrieving a document. It requires a human to connect each step. AI agents go further — they plan a sequence of actions, execute across connected systems, handle ambiguity, and adapt based on outcomes. The difference is between a calculator and a capable colleague who can carry out a complex, multi-step task independently.
Can AI agents make clinical decisions?
AI agents can produce structured, evidence-backed clinical recommendations — synthesising patient data, genomic information, current guidelines, and published evidence into a decision-ready output. However, responsible deployment in clinical settings always involves human oversight at high-stakes decision points. Agents in clinical environments are designed to support and accelerate the clinician's decision, not replace it.
What are multi-agent systems in cancer research?
Multi-agent systems are networks of specialised AI agents working in coordination. In cancer research, a multi-agent framework might include a literature agent, a genomics agent, a pathology agent, and a clinical guidelines agent — each handling its domain, with an orchestrator combining their outputs into a coherent, unified recommendation. This mirrors how a multidisciplinary clinical team works, but at a speed and scale no human team can match.
How do AI agents help with drug discovery?
AI agents automate the multi-step workflows of drug discovery: retrieving and synthesising relevant literature, generating molecular candidates, simulating compound behaviour against cancer targets, ranking leads by predicted efficacy and safety, and producing structured reports for experimental validation. They do not replace the scientist's judgment — they radically expand the search space a scientist can explore and compress the time between hypothesis and testable candidate.
What are the limitations of AI agents in oncology?
The main limitations are data quality requirements (agents are only as good as the data they can access), explainability constraints (clinical agents must show their reasoning, not just produce outputs), the need for human-in-the-loop design for high-stakes decisions, regulatory frameworks that are still maturing, and the integration complexity of connecting agents to live clinical systems. These are solvable engineering and governance challenges, not fundamental barriers — but they require deliberate architecture.
How do AI agents handle patient data securely?
Responsible agentic AI platforms for healthcare operate within HIPAA-compliant infrastructure, with every PHI access logged and permission-controlled. This includes SOC 2 Type II and ISO 27001 certification, on-premise or private cloud deployment options, de-identification protocols, and full audit trails for every agent action. Healthcare organisations should require these certifications from any AI agent vendor before deployment — not as a checkbox, but as evidence of architectural compliance.
Are AI agents being used in hospitals and healthcare operations today?
Yes. Production deployments of AI agents in healthcare are live across a range of operational use cases: healthcare staffing and scheduling automation, clinical program operations analytics, patient workflow orchestration, revenue cycle management, and administrative workflow automation. The research and academic literature on agents in clinical decision support is also growing rapidly, with clinical pilots transitioning to scaled deployments through 2025 and 2026.
What is precision oncology and how do AI agents support it?
Precision oncology is the practice of tailoring cancer treatment to the specific biological characteristics of an individual patient's tumour — its genomic variants, expression profile, and immune environment. AI agents support precision oncology by synthesising multi-modal patient data at a depth and speed that is not achievable manually: reading genomic sequencing results, cross-referencing clinical guidelines and trial data, and producing a structured, evidence-backed treatment recommendation that a clinician can review and act on.
What should I look for in an AI agent platform for healthcare?
Prioritise HIPAA-compliant architecture (not just policy), SOC 2 Type II and ISO 27001 certification, on-premise deployment capability, a governance layer that logs and permission-checks every agent action, genuine multi-agent orchestration, deep integration with clinical and operational systems, configurable human-in-the-loop controls, and documented production deployments in healthcare environments. Assistents by Ampcome meets all of these requirements and is already deployed in production across healthcare and life sciences operations.

Transform Your Business With Agentic Automation
Agentic automation is the rising star posied to overtake RPA and bring about a new wave of intelligent automation. Explore the core concepts of agentic automation, how it works, real-life examples and strategies for a successful implementation in this ebook.
Sarfraz Nawaz is the CEO and founder of Ampcome, which is at the forefront of Artificial Intelligence (AI) Development. Nawaz's passion for technology is matched by his commitment to creating solutions that drive real-world results. Under his leadership, Ampcome's team of talented engineers and developers craft innovative IT solutions that empower businesses to thrive in the ever-evolving technological landscape.Ampcome's success is a testament to Nawaz's dedication to excellence and his unwavering belief in the transformative power of technology.
More insights
Discover the latest trends, best practices, and expert opinions that can reshape your perspective



.webp)


Contact us

