
The Best AI Voice Agents for Healthcare in 2026: Compared, Ranked & Battle-Tested




Every day, a patient calls a clinic after hours. Nobody picks up. They wait on hold the next morning, give up after four minutes, and book with a competing provider instead.
That appointment slot goes unfilled. That revenue disappears. And the front-desk team that could have saved it was too busy handling three other calls simultaneously.
This is not an edge case. According to industry data, up to 60% of inbound healthcare calls go unanswered during peak hours or outside office hours — and 85% of patients who hang up will not leave a voicemail. They simply call the next option on their list.
AI voice agents in healthcare exist to close this gap. They handle inbound and outbound calls around the clock, understand natural patient language, complete real tasks — scheduling, triage, follow-ups, staffing intake — and do it without hold times, without fatigue, and without adding headcount.
This guide breaks down what these systems actually are, how they work, where they deliver measurable ROI, and what real enterprise deployments look like at scale.
What Are AI Voice Agents in Healthcare?
An AI voice agent in healthcare is an intelligent software system that conducts natural, spoken conversations with patients, staff, or facility operators — and takes real actions as a result.
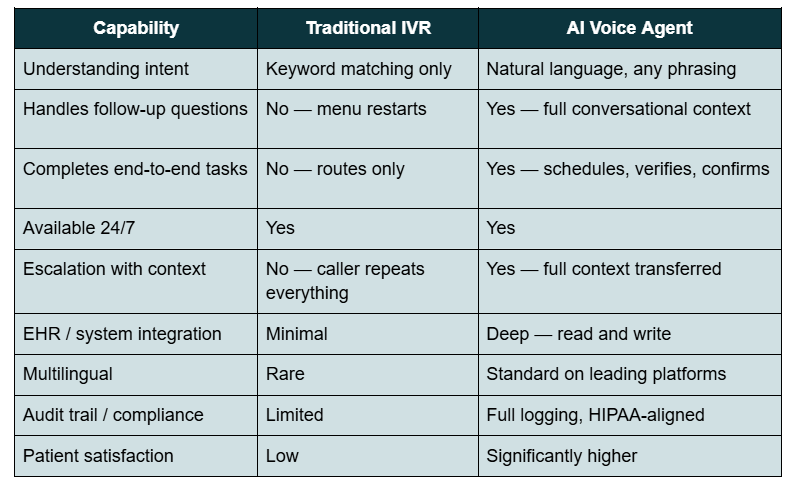
It is not a phone tree. It is not a menu-driven IVR. It understands intent, handles follow-up questions mid-conversation, and completes end-to-end tasks: booking an appointment, verifying insurance eligibility, routing a staffing request to the right facility, or following up with a patient post-discharge.
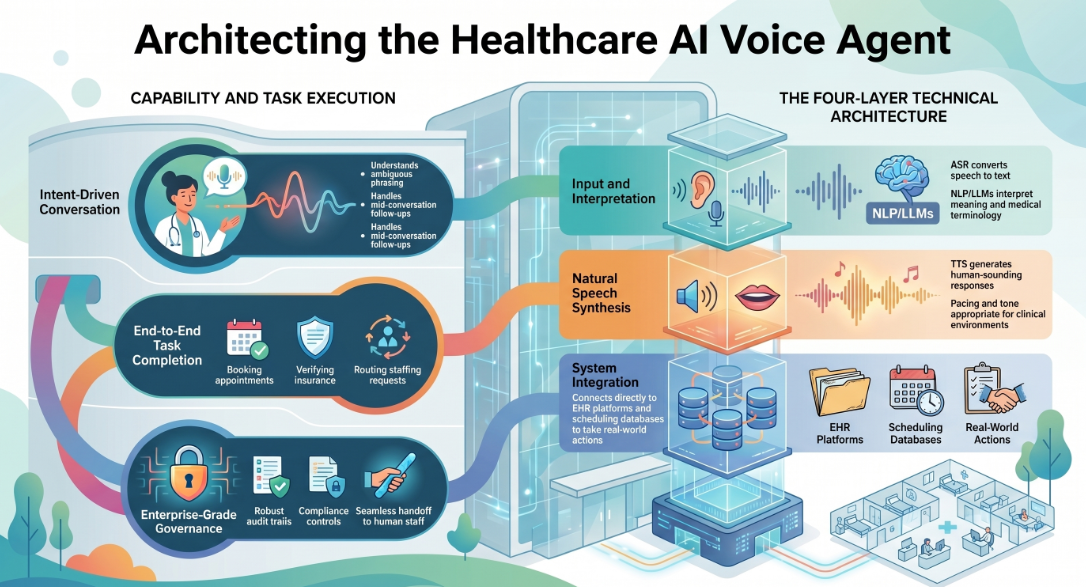
At a technical level, a healthcare AI voice agent runs on three core layers:
Automatic Speech Recognition (ASR): Converts spoken language into text in real time, with high accuracy on medical terminology, medication names, and insurance identifiers.
Natural Language Processing (NLP) + Large Language Model (LLM): Interprets what the caller means — not just what they say. Handles ambiguous phrasing, mid-sentence corrections, and multi-step requests without losing context.
Text-to-Speech (TTS) synthesis: Generates a natural, human-sounding spoken response with appropriate pacing, tone, and cadence.
Modern platforms add a fourth layer: system integration. The agent connects directly to EHR platforms (Epic, Cerner), scheduling systems, staffing databases, and CRM or compliance tools — so it doesn't just answer questions, it acts on them.
What separates enterprise-grade AI voice agents from consumer-grade bots is governance: audit trails, escalation logic, compliance controls, and the ability to hand off to a human at exactly the right moment with full context preserved.
Why Healthcare Needs AI Voice Agents Right Now
The pressure on healthcare operations is structural, not cyclical. Three converging forces are making AI voice agents not just useful, but necessary.
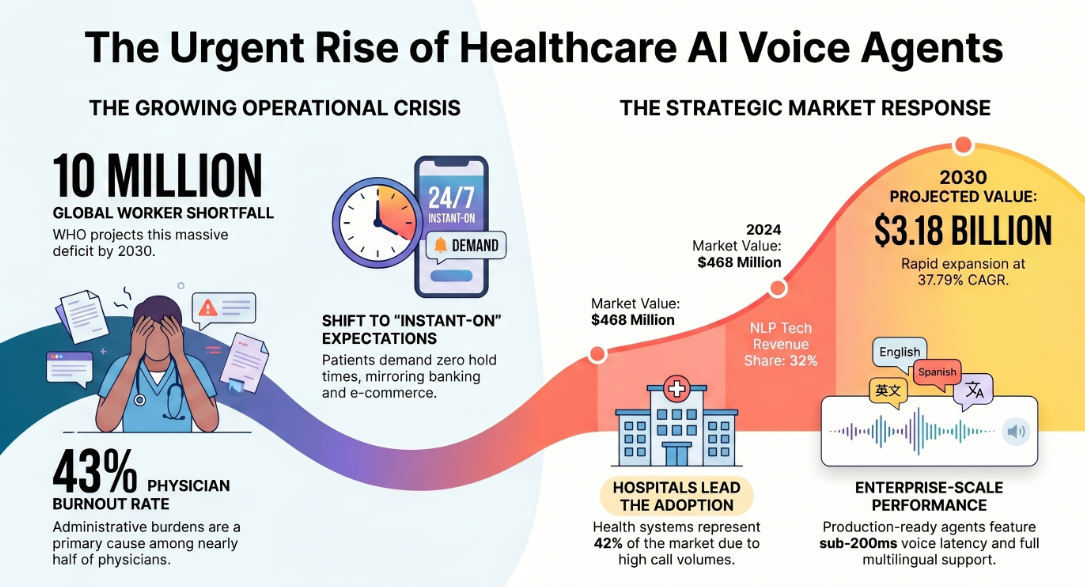
The staffing crisis is not going away. The WHO projects a global shortfall of 10 million healthcare workers by 2030. In the United States alone, the physician deficit is expected to reach 86,000 by 2036. The American Medical Association (AMA) reported in 2024 that 43% of physicians experienced at least one symptom of clinical burnout — with administrative burden cited as a leading cause. Every call a clinician or front-desk coordinator handles manually is time taken from patient care.
Patient expectations have shifted permanently. Patients now expect the same instant, 24/7 responsiveness from their healthcare provider that they get from banking or e-commerce. After-hours availability, same-session booking, and zero hold times are no longer premium experiences — they are baseline expectations.
The market is moving fast, and laggards are already behind. According to Grand View Research (2025), the global AI voice agents in healthcare market was valued at $468 million in 2024 and is projected to reach $3.18 billion by 2030, growing at a CAGR of 37.79%. NLP-powered conversational agents led the technology segment with a 32% revenue share in 2024. Hospitals and health systems account for the largest end-use segment at nearly 42% of the market — because they face the highest call volumes and the most complex workflow requirements.
Production deployments are now the baseline for serious vendor evaluation. If a platform cannot show you a named production customer at your scale, it is still in the pilot category.
Assistents.ai deploys governed AI agents — including Voice AI, Conversational Agents, Document AI, and Agentic BI — across healthcare, finance, logistics, and enterprise operations. With sub-200ms voice latency, multilingual support, and full audit trails, Assistents is built for organisations that need AI to operate at enterprise scale — not just pass a demo.
[Explore the Assistents Voice AI platform →]
How AI Voice Agents Work in a Healthcare Context
Understanding the architecture helps healthcare IT and operations leaders evaluate platforms with precision — and avoid the pilots that never make it to production.
The call path. A patient calls your main number. Instead of a hold queue or IVR menu, the AI voice agent answers in under one second. It identifies the caller's intent through natural language (not keyword matching), pulls relevant context from integrated systems, and begins completing the task conversationally. If the call requires clinical judgment, urgency escalation, or a scenario outside its governed parameters, it transfers to a live agent with full call context — no repeat explanations.
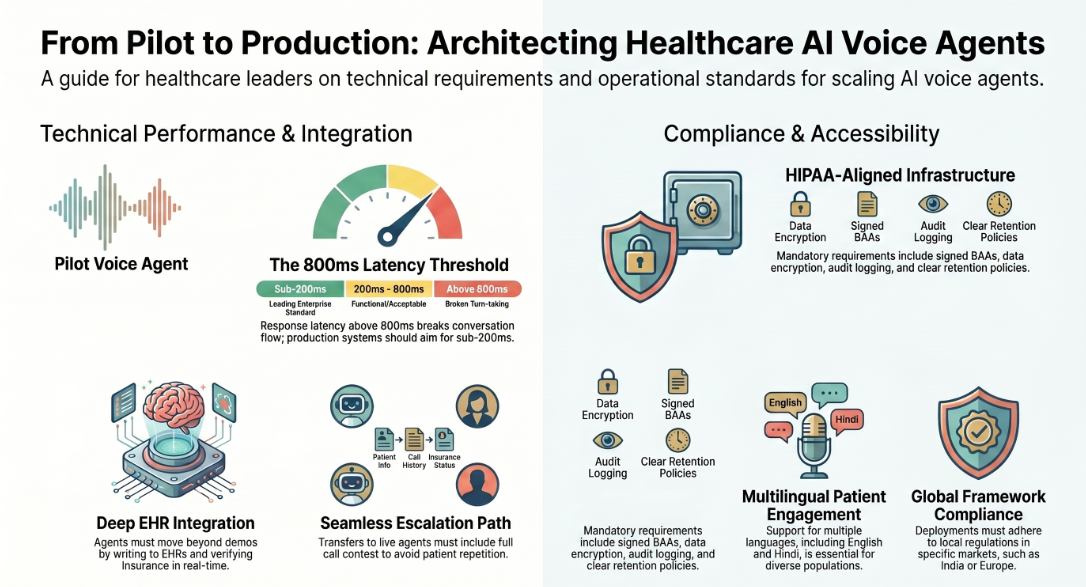
Latency matters more than most vendors admit. Above approximately 800 milliseconds of response latency (p99), turn-taking in voice conversations feels broken to the caller. Enterprise platforms measure and publish real p99 latency on production traffic — not marketing p50 numbers. Sub-200ms latency on the response layer is achievable and should be a requirement in any vendor evaluation.
EHR integration is where pilots fail. The gap between a proof-of-concept demo and a production healthcare voice agent almost always comes down to integration depth. Can the agent write back to the EHR after scheduling? Can it verify insurance in real time against a live payer database? Can it access a staffing platform to check credential status before confirming a shift? Seams in the call path — AI to telephony, AI to EHR, AI to compliance system — are where pilot-stage platforms break down at scale.
Compliance is non-negotiable. Any healthcare voice agent handling protected health information (PHI) must operate under HIPAA-aligned infrastructure. This means a Business Associate Agreement (BAA) with the vendor, encrypted data in transit and at rest, audit logging of every interaction, and clearly defined data retention policies. For deployments in India or other regulated markets, equivalent local frameworks apply.
Multilingual capability is a competitive differentiator, not a nice-to-have. In diverse patient populations — and particularly in markets like India — a voice agent that only handles English will leave significant patient engagement and operational value on the table. Leading platforms support Hindi, English, and multiple other languages with near-native quality.
Core Use Cases: Where AI Voice Agents Deliver Real ROI in Healthcare
1. Patient Scheduling and Intake
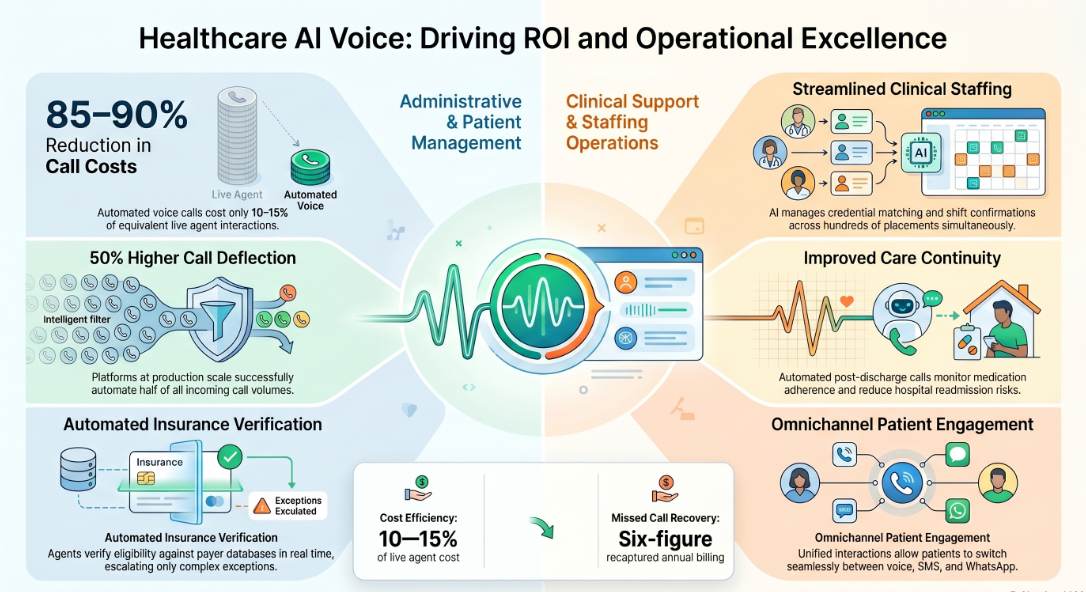
The most immediate and measurable use case. AI voice agents handle inbound scheduling calls, collect intake information, confirm appointment details, send reminders, and manage rescheduling — across every hour of the day, including evenings, weekends, and holidays.
The ROI is direct: automated voice calls cost 10–15% of equivalent live agent calls, and platforms operating at production scale achieve 50% or higher call deflection rates. At a mid-size private practice receiving several hundred calls per month, missed call recovery alone can translate to six figures in recaptured annual billing.
2. Healthcare Staffing Operations
This is one of the least discussed but highest-value applications of AI voice in healthcare. Staffing platforms connecting nursing professionals and other clinical staff to healthcare facilities face enormous operational complexity: matching credentials to facility requirements, confirming shift availability, managing last-minute changes, and maintaining compliance documentation.
AI voice agents handle the intake, matching communication, scheduling confirmations, and compliance notification calls at scale — without the manual overhead of a staffing coordinator making individual calls across hundreds of placements. Faster fill cycles, better utilisation, and dramatically lower scheduling friction are the consistent outcomes of live deployments in this space. (See the deployment case study below.)
3. Inpatient and Post-Discharge Follow-Up
Physician-led inpatient programs — hospitalist services, geriatric care programs, post-acute coordination — generate substantial outbound communication volume. Discharge follow-up calls, medication adherence checks, care plan confirmations, and appointment booking post-stay are high-volume, time-sensitive, and largely routine in content.
AI voice agents manage this outbound communication consistently, at scale, and flag non-standard responses for clinician review. The result: improved care continuity, reduced readmission risk, and better visibility into program performance — without adding clinical headcount.
4. Omnichannel Patient Follow-Up and Engagement
Modern patients move between channels — voice, WhatsApp, SMS, web chat — often within a single care journey. Enterprise-grade AI voice platforms support omnichannel continuity: a patient can start a conversation via voice, continue it on WhatsApp, and receive a confirmation by SMS — with the agent maintaining full context across channels and a unified interaction record.
For healthcare providers managing high volumes of ongoing patient relationships (chronic disease management, post-operative follow-up, preventive care outreach), this continuity is the difference between AI that merely answers calls and AI that actually drives patient engagement at scale.
5. Insurance Verification and Administrative Automation
Insurance verification, prior authorisation, billing inquiries, and claims status calls are high-volume, low-complexity interactions that consume significant staff time. AI voice agents handle these workflows end-to-end — verifying eligibility in real time against payer databases, walking patients through coverage details, and escalating to billing staff only when exceptions arise.
AI Voice Agents vs. Traditional IVR: A Direct Comparison
Real Deployments: What Actual Results Look Like
The following case studies are drawn from live enterprise deployments in healthcare. Client names are not disclosed.
Case Study 1: AI Voice Agent for a Healthcare Staffing Platform
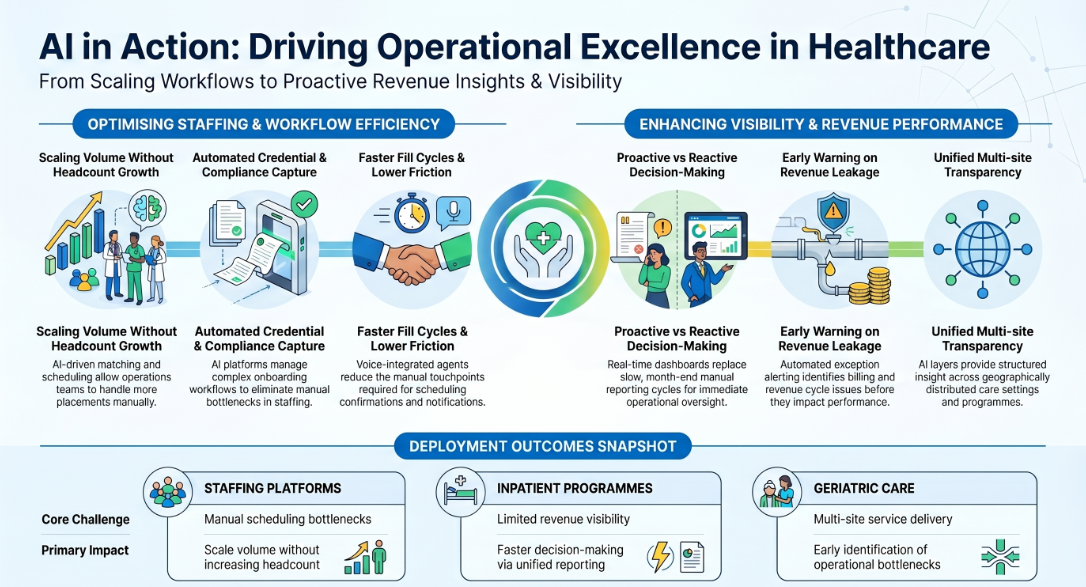
The challenge. A US-based healthcare staffing platform connecting nursing professionals with healthcare facilities faced a scaling problem. Matching, scheduling, and compliance workflows were being managed manually — creating bottlenecks, delayed fill cycles, and high operational overhead as the platform grew.
What was deployed. A comprehensive AI platform for healthcare staffing operations, covering talent onboarding and credential capture, facility staffing request intake and matching logic, scheduling confirmation and notifications via voice, and compliance workflow management. Reporting dashboards tracking fill rates and workforce utilisation were layered on top.
Results. Faster fill cycles and significantly lower scheduling friction. Improved workforce utilisation across the platform. Better staffing responsiveness for healthcare facilities — with fewer manual touchpoints per placement. The operations team was able to scale placement volume without proportionally scaling headcount.
Case Study 2: Operational and Revenue Analytics for a Physician-Led Inpatient Program
The challenge. A physician-led clinical enterprise operating hospitalist programs across a regional health system had limited visibility into care program performance and financial outcomes. Manual reporting cycles were slow and inconsistent, and the team lacked real-time tools to identify operational bottlenecks before they affected revenue or care quality.
What was deployed. A data analytics and voice-integrated agent layer covering revenue and utilisation analytics, performance dashboards with variance explanations, exception alerting for revenue cycle issues, and operational workflow support for inpatient coordination. Action lists were generated automatically to guide billing workflow improvements.
Results. Improved visibility into revenue leakage drivers. Faster operational decision-making through unified reporting. More reliable tracking of program performance across care settings. Leadership gained the real-time oversight to make proactive decisions on staffing, billing, and care delivery — rather than reacting to month-end reports.
Case Study 3: AI for Geriatric Care Program Performance
The challenge. A geriatric care services provider in a major US metro area — delivering physician-led programs across assisted living and long-term care settings — needed better tools to manage program operations, staffing, and service delivery analytics across a geographically distributed model.
What was deployed. Program operations dashboards, staffing and service delivery analytics, and revenue cycle visibility with exception alerts. The AI layer surfaced performance bottlenecks, flagged service delivery gaps, and provided leadership with consistently structured insight across care programs.
Results. Faster identification of operational bottlenecks. Improved transparency into service performance across care settings. Better decision support for leadership teams managing multi-site operations. More consistent revenue cycle tracking with early warning on exception scenarios.
What to Look for in a Healthcare AI Voice Agent: Evaluation Checklist
Not all voice AI platforms are built for healthcare. Here is a practical framework for evaluating options:
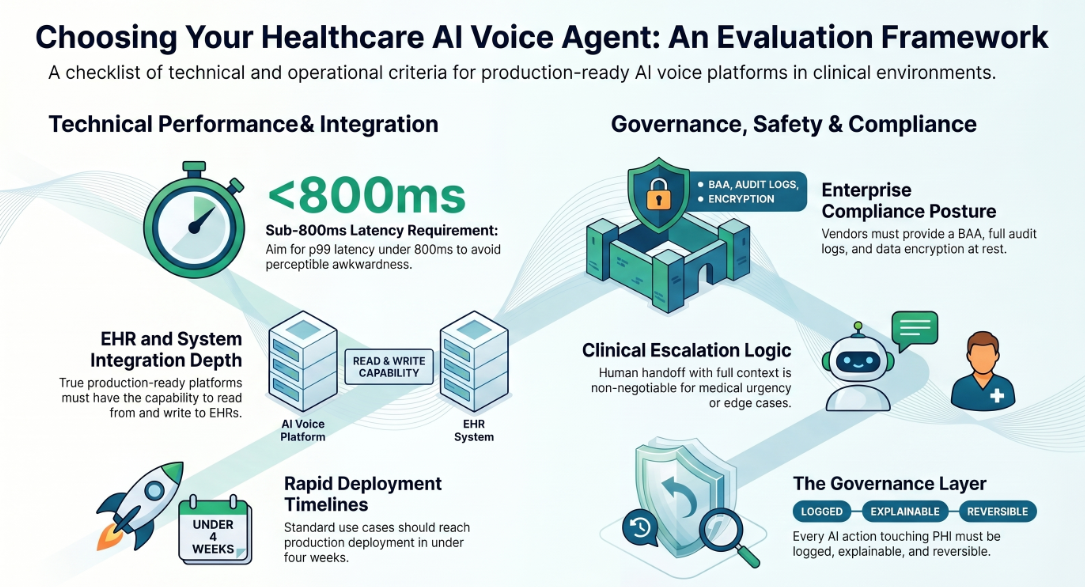
Latency. Request real p99 latency numbers on production traffic. Anything above 800ms creates perceptible awkwardness in voice conversations. Sub-200ms on the TTS response layer is achievable.
EHR and system integration depth. Can the agent read from and write to your EHR? Can it verify insurance against live payer data? Does it integrate with your staffing platform, CRM, or compliance tools? Integration depth is the primary differentiator between pilot-stage and production-ready platforms.
Compliance posture. Does the vendor offer a BAA? Is data encrypted in transit and at rest? Are full audit logs available per interaction? What is the data retention policy?
Multilingual capability. If your patient population or operational staff require multiple languages, verify native (not translated) language support. For India deployments specifically, Hindi and regional language support is essential.
Escalation logic. How does the agent handle edge cases, medical urgency, or conversations outside its governed parameters? Human handoff with full context is non-negotiable in a clinical setting.
Omnichannel continuity. Can the agent maintain context across voice, WhatsApp, SMS, and web chat? Is there a unified interaction record across channels?
Governance and auditability. In healthcare, every AI action that touches PHI or drives a clinical workflow needs to be logged, explainable, and reversible. Platforms without a governance layer are not suitable for enterprise healthcare deployment.
Time to production. Proof-of-concept to production deployment in under four weeks is achievable with the right platform. If a vendor's implementation timeline exceeds 90 days for a standard use case, ask why.
AI Voice Agents for Healthcare in India: A Fast-Growing, Underserved Opportunity
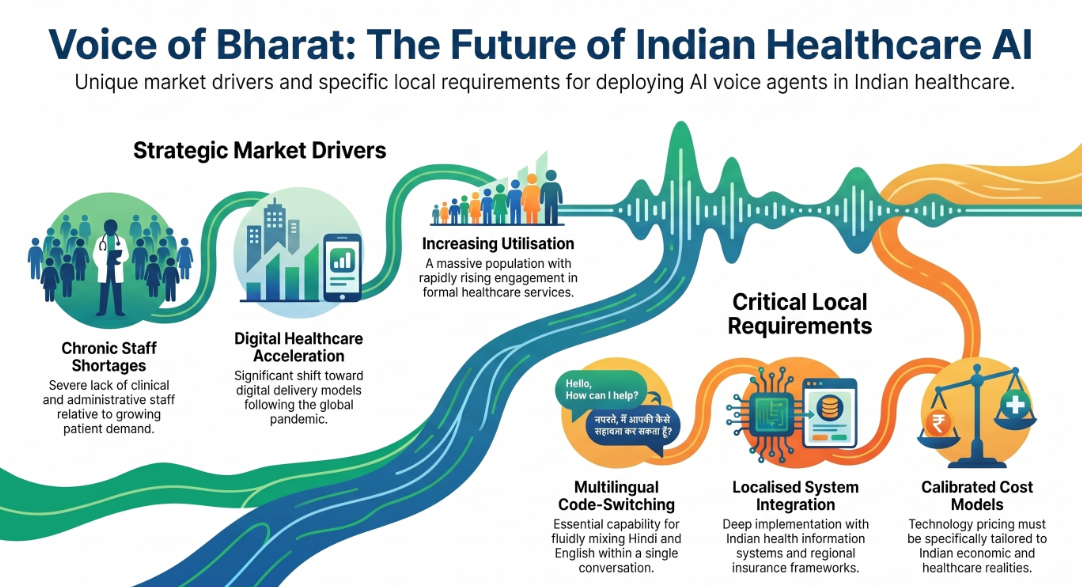
India represents one of the fastest-growing markets for healthcare AI voice deployment — and one of the most underserved in terms of purpose-built solutions.
The structural drivers are significant: a large and growing population with increasing healthcare utilisation, a chronic shortage of clinical and administrative staff relative to demand, a diverse multilingual patient base spanning Hindi, English, and dozens of regional languages, and an accelerating shift toward digital healthcare delivery post-pandemic.
The specific requirements for effective healthcare AI voice deployment in India differ from Western markets in meaningful ways. Multilingual fluency — particularly Hindi and English code-switching within a single conversation — is essential, not optional. Integration with Indian health information systems and regional insurance frameworks requires local implementation expertise. And the cost model for healthcare AI in India must be calibrated to local pricing realities.
Live healthcare AI deployments in India — including enterprise-scale implementations in clinical operations, health infrastructure, and staffing — have demonstrated that the technology works in this context. The critical variables are integration depth, language quality, and governance posture. Platforms that treat India as a geographic afterthought — offering an English-only, US-infrastructure product with a local sales layer — will not deliver production-grade results.
What Does It Actually Cost? A Simple ROI Framework
Healthcare leaders evaluating AI voice agents often ask the same first question: what is the return, and how quickly does it materialise?
Here is a straightforward framework for a mid-size healthcare operation:
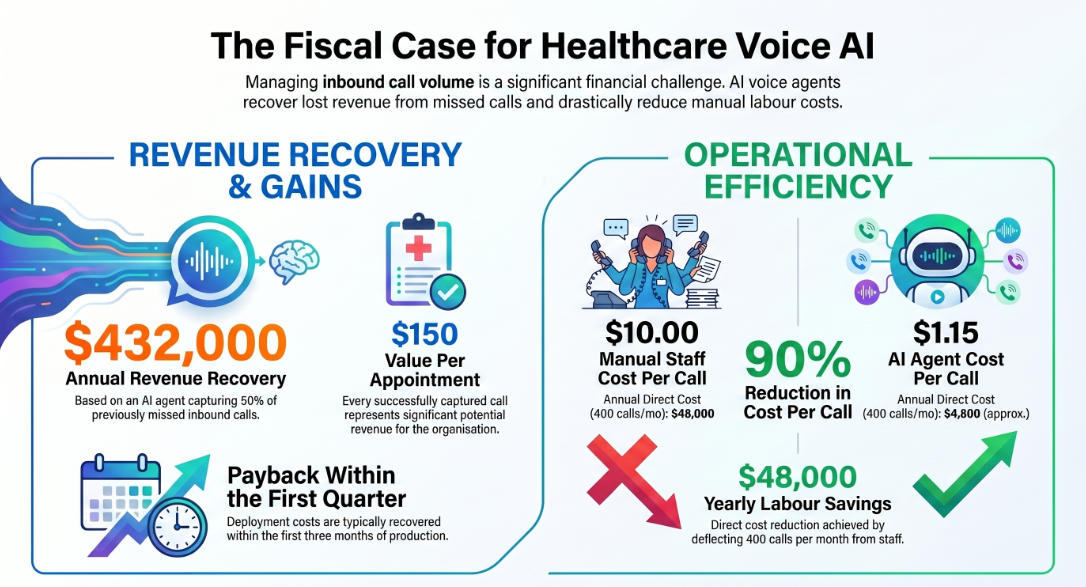
Baseline assumptions:
- 800 inbound calls per month
- 60% missed or poorly handled during peak and after-hours
- Average value of a captured appointment: $150
- Current cost per manually handled call: $8–12 (staff time)
- AI voice agent cost per handled call: $0.80–$1.50
Recovery scenario: If the AI voice agent captures 50% of previously missed calls (240 per month), that represents $36,000 in recovered monthly revenue, or $432,000 annually — before accounting for reduced staff burden on the calls the agent fully deflects.
Deflection value: If the agent fully handles 400 calls per month that previously required staff time at $10 per call, that is $4,000 per month in direct labour cost reduction, or $48,000 annually.
Total first-year value (conservative): $480,000+
These numbers are illustrative and will vary based on call volume, appointment value, and current staffing model. The point is that the ROI calculation for healthcare voice AI is not complex — and for most organisations operating at meaningful call volume, payback occurs within the first quarter of production deployment.
Getting Started: What a Production Deployment Actually Looks Like
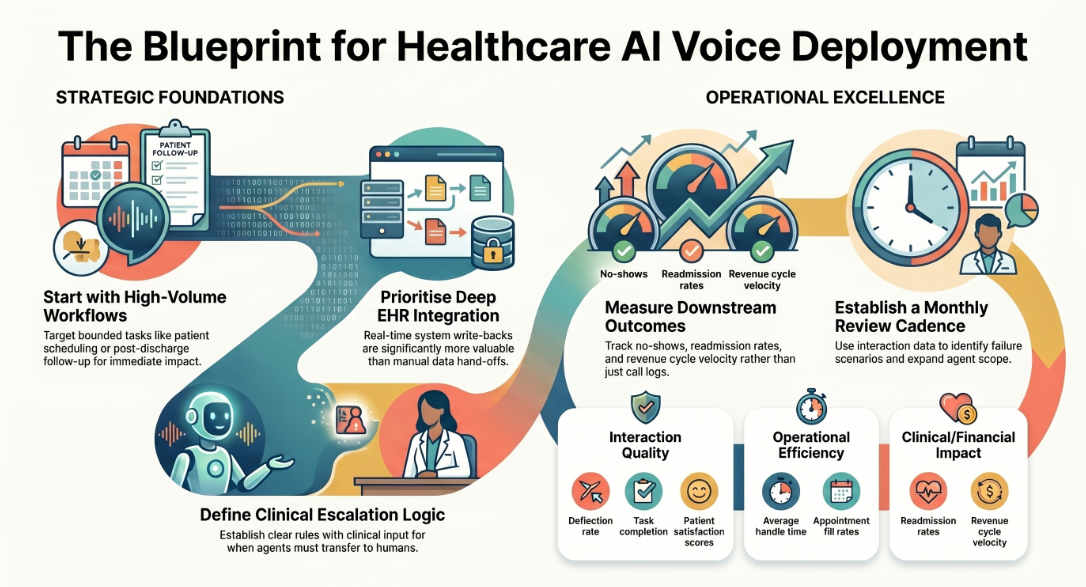
Healthcare leaders who have moved from pilot to production on AI voice share a consistent set of observations:
Start with a contained, high-volume workflow. Patient scheduling or post-discharge follow-up are ideal first deployments — measurable, bounded, and immediately impactful. Avoid starting with edge-case-heavy workflows like complex insurance disputes or clinical triage.
Invest in integration quality upfront. The ROI on deep EHR and system integration is disproportionate. A voice agent that can actually write back to the scheduling system and confirm in real time is categorically more valuable than one that collects information and hands it off for manual entry.
Define escalation logic before launch. Every healthcare voice deployment needs clearly defined rules for when and how the agent transfers to a human. These rules should be built with clinical and operations input, not left to default platform settings.
Measure what matters. Track call deflection rate, task completion rate, average handle time, patient satisfaction score on AI-handled calls, and — most importantly — downstream outcomes: no-shows, readmissions, fill rates, revenue cycle velocity. The agent's performance is visible in operational data, not just call logs.
Plan for continuous improvement. Production AI voice agents improve with interaction data. Establish a monthly review cadence to identify high-frequency failure scenarios, update governing rules, and expand the agent's scope as confidence grows.
The Bottom Line
AI voice agents in healthcare are no longer a future-state technology. They are in production across staffing platforms, physician-led inpatient programs, geriatric care services, hospital systems, and multi-site clinical enterprises — handling real patient interactions, real staffing workflows, and real operational tasks at scale.
The organisations that deploy thoughtfully — with integration depth, governance posture, and clear success metrics — are recovering missed revenue, reducing administrative burden, and delivering consistent patient and staff experiences that manual operations cannot match.
The gap between a voice AI pilot and a production deployment in healthcare comes down to three things: integration depth, compliance architecture, and the willingness to treat the agent as a governed operational system rather than a chatbot with a phone number.
If you are evaluating AI voice agents for healthcare — whether for a staffing platform, an inpatient program, a multi-site clinical enterprise, or a regional hospital — the right question is not "does this technology work?" The question is "which implementation approach will get us to production, measurable ROI, and operational confidence within 90 days?"
FAQs
What is the best AI voice agent for hospitals?
The best AI voice agent for a hospital depends on integration requirements, call volume, and compliance needs. Key differentiators to evaluate are EHR integration depth, HIPAA compliance posture, multilingual support, and real p99 latency on production deployments. Platforms like Assistents.ai are built specifically for enterprise healthcare environments requiring governance, auditability, and omnichannel continuity — not just call deflection.
Are AI voice agents HIPAA compliant?
HIPAA compliance in AI voice is not automatic — it is a product and infrastructure decision by the vendor. A HIPAA-compliant AI voice agent requires: a signed Business Associate Agreement (BAA) with the vendor, PHI encryption in transit and at rest, full audit logging of every interaction, and documented data retention and deletion policies. Always request BAA terms and a compliance documentation package before any production deployment.
How do AI voice agents differ from IVR systems?
Traditional IVR systems route callers through pre-set menu options using keyword detection. AI voice agents understand natural language, handle any phrasing of a request, maintain conversational context across multiple exchanges, integrate with backend systems to take real actions (scheduling, verification, staffing), and escalate to humans with full context when needed. The patient experience difference is significant: IVR deflects; AI voice resolves.
How much do AI voice agents cost for healthcare?
Pricing models vary by vendor and typically depend on call volume, feature set, and integration complexity. Cost per handled call on AI voice ranges from approximately $0.80 to $1.50 — compared to $8–12 per manually handled call at equivalent staff cost. Most enterprise platforms offer usage-based pricing with volume tiers. Total implementation costs depend on integration depth and customisation requirements.
Can AI voice agents handle multilingual healthcare conversations?
Leading enterprise platforms support multilingual voice conversations natively — including Hindi and English for India-based deployments, as well as other languages. The key distinction is native language support (model trained on the language) versus translation-layer support (real-time machine translation). For patient-facing healthcare use cases, native language support is strongly preferred for accuracy on medical terminology and natural conversational flow.
How long does it take to deploy a healthcare AI voice agent?
Well-architected platforms with pre-built healthcare integrations can reach production in under four weeks for standard use cases. More complex deployments involving deep EHR integration, custom compliance workflows, or multi-site rollouts typically require 6–12 weeks. Treat any vendor quoting six months or more for a standard deployment as a red flag.
What workflows are best suited to AI voice agents in healthcare?
High-volume, rule-governed, time-sensitive workflows are the ideal starting point: inbound scheduling and rescheduling, post-discharge follow-up calls, insurance and eligibility verification, healthcare staffing intake and shift confirmation, medication adherence outreach, and appointment reminders. As governance confidence grows, the scope expands to more complex multi-step workflows.

Transform Your Business With Agentic Automation
Agentic automation is the rising star posied to overtake RPA and bring about a new wave of intelligent automation. Explore the core concepts of agentic automation, how it works, real-life examples and strategies for a successful implementation in this ebook.
Sarfraz Nawaz is the CEO and founder of Ampcome, which is at the forefront of Artificial Intelligence (AI) Development. Nawaz's passion for technology is matched by his commitment to creating solutions that drive real-world results. Under his leadership, Ampcome's team of talented engineers and developers craft innovative IT solutions that empower businesses to thrive in the ever-evolving technological landscape.Ampcome's success is a testament to Nawaz's dedication to excellence and his unwavering belief in the transformative power of technology.
More insights
Discover the latest trends, best practices, and expert opinions that can reshape your perspective



.jpg)



Contact us

