
How AI for Medical Prior Authorization Is Eliminating the Approval Bottleneck (2026 Guide)




A physician finalizes a treatment plan. Medical necessity is established. The care pathway is clear.
And then everything stops.
The request sits in a payer review queue, waiting on documentation that already exists, reviewed against criteria that are already met. Staff make follow-up calls. Patients wait. Days pass. In some cases, patients abandon care entirely.
Prior authorization was designed to control costs and ensure appropriate treatment. Instead, it has become one of the most resource-draining, care-delaying processes in modern healthcare. The American Medical Association has found that over 78% of physicians say prior authorization delays cause patients to abandon recommended care. Over 25% report it has led to serious adverse patient events.
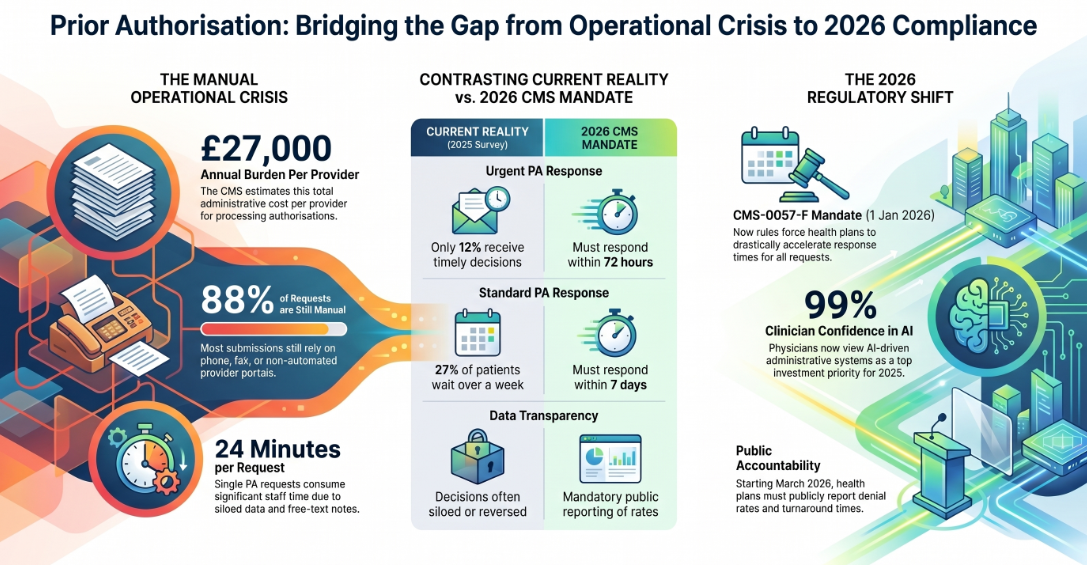
The administrative cost to providers sits at an estimated $34,000 per provider annually, according to CMS data. And the system processing these requests — for the most part — is still built on phone calls, faxes, and manual form submissions.
That is the problem. AI for medical prior authorization is increasingly the solution — but not all AI is solving it the right way.
This guide covers what is actually broken, what agentic AI does differently, how the full automation workflow operates, real-world results across healthcare operations, and what the CMS 2026 compliance mandate means for every provider and health plan that has not yet acted.
What Is Medical Prior Authorization (And Why It Is Still Broken)
Prior authorization, or prior auth, is the process by which a healthcare provider must obtain advance approval from a patient's insurance company before delivering certain treatments, procedures, medications, or services. Insurance companies use it to verify medical necessity and manage costs.
In principle, it is a reasonable system. In practice, it has become healthcare's most contentious administrative bottleneck.
The Administrative Cost Nobody Talks About
Processing a single prior authorization request consumes up to 24 minutes of staff time, according to Waystar's research. Multiply that across tens of millions of authorizations annually, and the math becomes catastrophic for operations teams. CMS estimates the total administrative burden at $34,000 per provider per year.
That is not a billing inefficiency. That is an operational crisis.
Why 88% of Prior Authorization Requests Were Still Manual
As recently as 2019, 88% of prior authorization submissions were still processed manually — through phone, fax, or provider portals with no automation. Despite the availability of Electronic Prior Authorization (ePA) frameworks, adoption has been slow because most EHR and billing systems treat PA as a siloed step rather than an integrated workflow.
The data required for a PA submission does not live in one place. Physician notes exist in free-text fields. Lab results are separate attachments. Imaging reports sit in diagnostic systems that rarely communicate with billing platforms. Payer policy documents are updated continuously and stored in formats that legacy systems cannot parse in real time.
Standard software automation cannot handle this. It was not built to.
The CMS 2026 Interoperability and Prior Authorization Final Rule
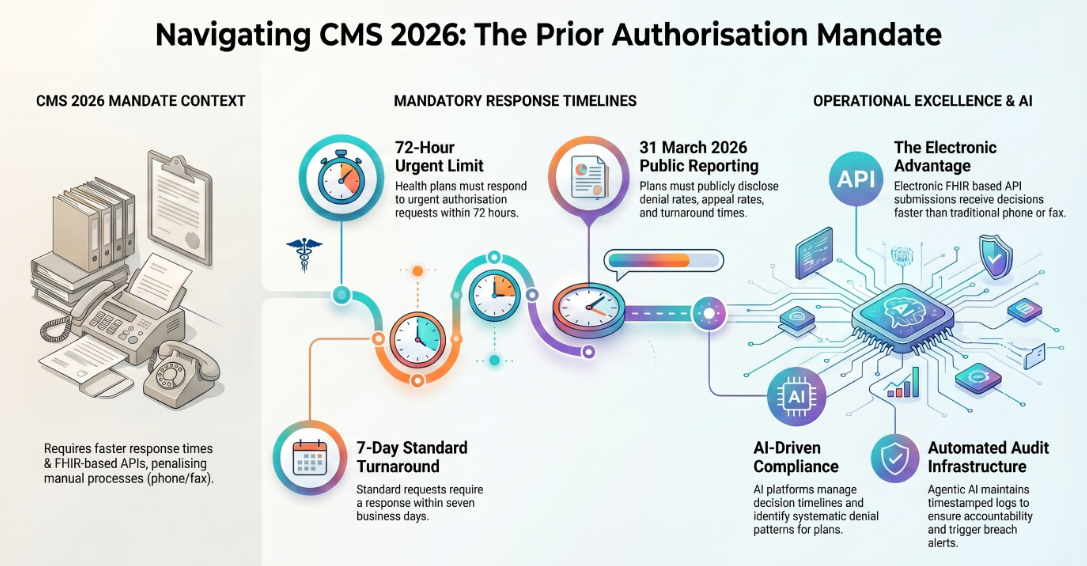
The regulatory pressure is now forcing the issue. The CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F), which took effect January 1, 2026, mandates that all covered health plans:
- Respond to urgent prior authorization requests within 72 hours
- Respond to standard prior authorization requests within 7 days
- Publicly report their average turnaround times, denial rates, appeal rates, and overturn rates on their websites starting March 31, 2026
The gap between what the mandate requires and what providers currently experience is severe. Only 12% of clinicians and 7% of office administrators report that they consistently receive PA decisions within those timeframes today, according to Cohere Health's 2025 National Provider Survey.
Health plans that cannot demonstrate compliance will face public scrutiny at a level the industry has not seen before. Providers who remain on manual workflows will absorb the full cost of that gap.
What the Physician Community Is Saying
The pressure from the clinical side is equally stark. A 2025 national survey by the PAN Foundation found that 27% of patients waited over a week for an insurance decision, and 34% experienced a reversal on an initially approved authorization. Physicians are not just frustrated — 47% of them rank automated administrative systems as a top investment priority for 2025, according to Innovaccer's AI Trends in Healthcare report.
Trust in AI to handle this is no longer a hesitation point. Cohere Health's 2025 National Provider Survey found that 99% of clinicians and 96% of office administrators report confidence in AI-driven prior authorization. The question has shifted from "should we use AI for prior authorization?" to "which AI is actually doing the job end to end?"
What Traditional AI Tools Get Wrong About Prior Authorization
Most AI tools marketed for prior authorization are solving a subset of the problem, not the whole problem. Understanding the difference matters before selecting a platform.
Point Solutions Versus End-to-End Workflow Agents
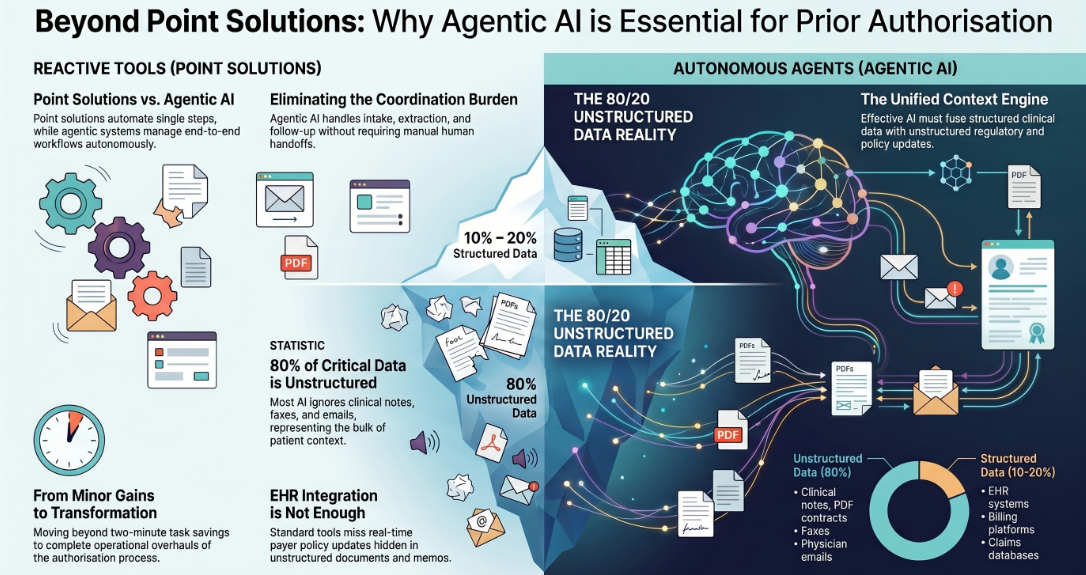
The majority of AI prior authorization products on the market today are point solutions. They automate one step — eligibility checks, form pre-fill, status monitoring — and hand off to a human for everything else. The coordination burden, the exception handling, the multi-system orchestration: those still fall on staff.
A point solution that saves two minutes per submission is a minor efficiency gain. An agentic AI system that handles intake, extraction, payer matching, submission, follow-up, and escalation end to end is an operational transformation.
The architectural difference is significant. Point solutions are reactive tools. Agentic AI systems are autonomous workflows that execute, adapt, and escalate without requiring manual handoffs between each step.
The 80/20 Data Problem in Prior Authorization
Most AI tools connect to structured data sources — EHR systems, claims databases, billing platforms — and treat that as sufficient context. It is not.
Structured data represents only 10 to 20% of what a healthcare organization actually knows about a patient at the moment of a prior authorization request. The other 80% lives in:
- Clinical notes in free-text fields
- PDF contracts containing payer-specific coverage terms
- Faxed referrals with critical patient history
- Physician emails clarifying treatment necessity
- Policy documents that change reimbursement rules quarterly
- Compliance memos distributed across SharePoint, email, and internal systems
An AI that cannot read, interpret, and act on that 80% will produce incomplete submissions, trigger denials, and require human correction — which is precisely the problem it was supposed to solve.
Why EHR Integration Alone Is Not Enough
EHR integration is necessary but not sufficient. A system that pulls structured patient data and pre-fills authorization forms is valuable, but payer rules change continuously. Formulary updates, coverage criteria revisions, and new medical necessity guidelines are published in unstructured documents that standard EHR-integrated tools do not ingest or apply in real time.
The result is a submission that was correct yesterday but fails today because the payer updated their clinical criteria two weeks ago and the system was never told.
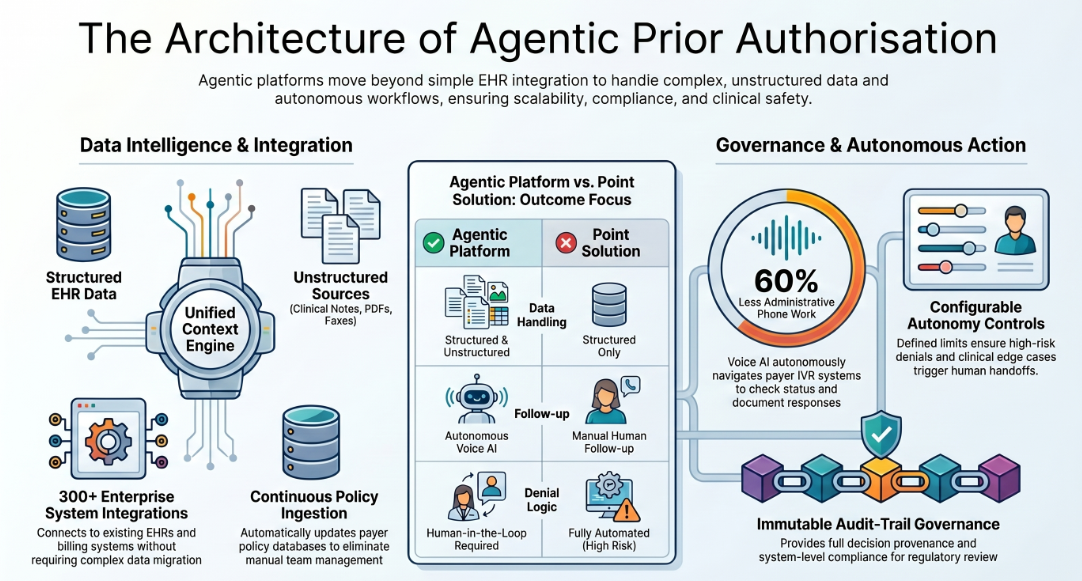
Effective AI for medical prior authorization requires a unified context engine that fuses structured clinical data with unstructured policy documents and external regulatory updates — and applies that complete context before every submission.
How Agentic AI Handles the Full Prior Authorization Workflow
Agentic AI does not automate a step. It automates the workflow — from the moment an authorization is needed to the moment a decision is received, tracked, and acted upon.
Here is how a complete agentic prior authorization workflow operates in practice.
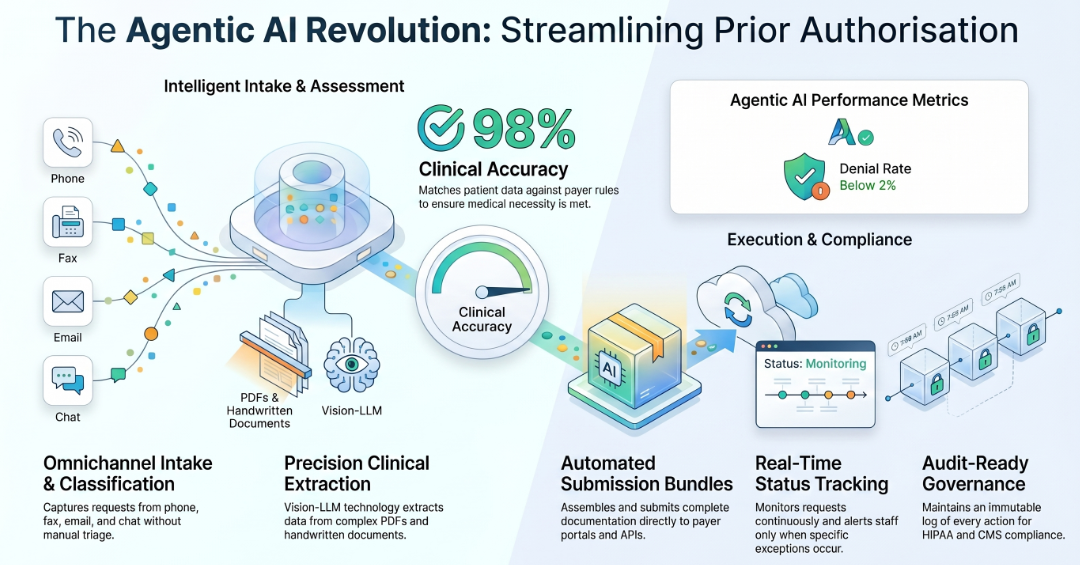
Step 1: Omnichannel Intake
Prior authorization requests do not arrive through a single channel. They come via phone, fax, provider portal, email, and increasingly through WhatsApp and chat interfaces. An agentic AI system captures intake across all of these channels simultaneously, classifies the request type, and routes it into the appropriate workflow — without any manual triage.
For voice-based payer follow-up calls, voice AI agents handle the conversation directly: asking for denial reasons, requesting peer-to-peer reviews, and documenting outcomes — all without a staff member on the line.
Step 2: Intent Classification and Clinical Data Extraction
Once intake is captured, the agent identifies what type of authorization is required, extracts the relevant clinical information from the patient record, and pulls supporting documentation from unstructured sources — including physician notes, prior imaging reports, lab values, and referral letters.
Vision-LLM technology enables extraction from complex PDFs, handwritten fax content, and scanned documents that standard OCR cannot reliably parse. This is the capability that closes the 80/20 data gap.
Step 3: Payer Rule Matching and Medical Necessity Assessment
The agent queries an up-to-date database of payer-specific clinical criteria, coverage policies, and formulary rules. It matches the extracted patient data against the applicable payer's current requirements and assesses whether the request meets medical necessity criteria.
Platforms operating with this architecture report prior authorization accuracy rates exceeding 98% and denial rates below 2%. For complex cases where criteria are not clearly met, the agent identifies the specific documentation gap and routes to a human reviewer with a structured brief — not a raw claim file.
Step 4: Automated Submission with Full Documentation Bundle
The agent assembles the complete prior authorization request — clinical summary, supporting documentation, coded fields, and medical necessity justification — and submits it directly to the payer through the appropriate channel: electronic portal, API integration, or standardized fax.
No staff member touches a form. No documentation is missing. No submission is delayed because a team member is on another call.
Step 5: Real-Time Status Tracking and Exception Alerting
Once submitted, the agent monitors the request continuously. Status updates are logged. Payer responses are captured. When an exception occurs — a request for additional information, a pending denial, a hold for peer review — the agent generates an alert with context and recommended action, routed to the appropriate team member.
This eliminates the reactive, labor-intensive follow-up cycle that consumes staff time across most prior authorization operations today.
Step 6: Human-in-the-Loop Escalation with Full Audit Trail
For decisions that require clinical judgment, appeal preparation, or payer escalation, the agent hands off to a human with full context: the original submission, payer communication history, denial reason codes, and suggested appeal language based on comparable approved cases.
Every action taken by the agent — every data extraction, every submission, every escalation decision — is logged in an immutable audit trail. This satisfies HIPAA compliance requirements and provides the documentation depth that CMS's new public reporting mandate demands.
Real-World Results: What AI-Driven Prior Authorization Automation Delivers
The outcomes described above are not theoretical. Agentic AI deployments across healthcare operations have produced measurable results across staffing, inpatient care, and multi-site clinical enterprises.
Healthcare Staffing Operations
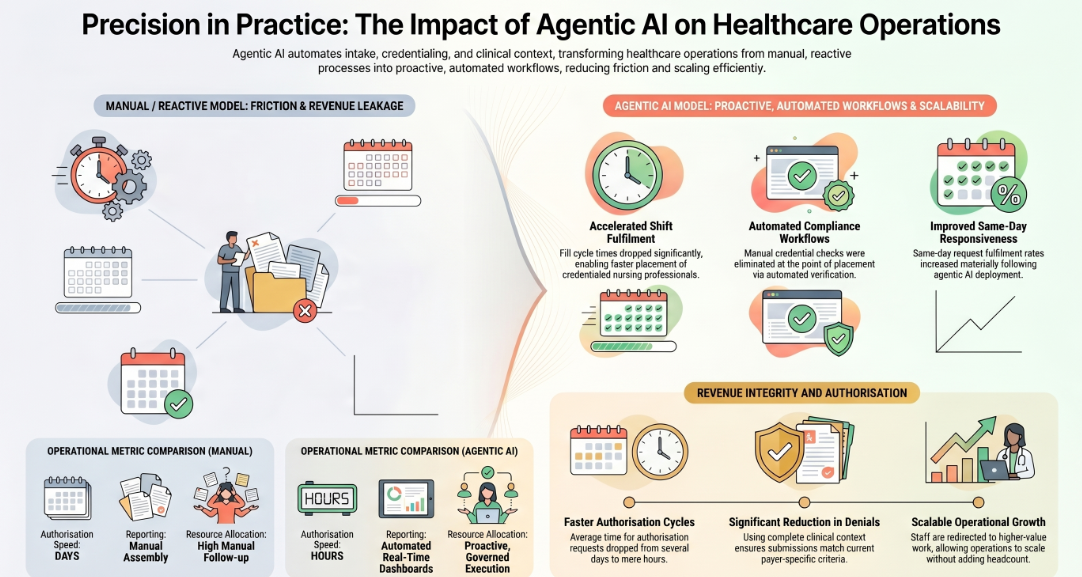
A healthcare staffing platform used by nursing professionals and healthcare facilities faced a core operational challenge: matching credentialed staff to authorized shift requests, while ensuring that facility-level compliance requirements were met before a placement was confirmed. Authorization delays created scheduling failures, compliance gaps, and revenue loss from unfilled shifts.
Following deployment of an agentic AI platform covering intake, credential verification, authorization matching, and scheduling coordination:
- Fill cycle times dropped significantly, reducing the scheduling friction that had been the primary cause of missed placements
- Staffing responsiveness to facilities improved materially, with same-day request fulfillment rates increasing
- Compliance workflow automation eliminated manual credential checks at the point of placement
- Reporting on fill rates, utilization, and compliance coverage moved from manual assembly to automated, real-time dashboards
The operational model shifted from reactive staffing coordination to proactive, governed execution — without adding headcount.
Inpatient and Geriatric Care Operations
A physician-led inpatient clinical enterprise operating hospitalist programs faced persistent challenges with revenue cycle visibility and authorization documentation across multiple facilities. Authorizations were tracked inconsistently, denial rates were above industry benchmarks, and the revenue cycle team lacked real-time visibility into where approvals were pending.
After deployment of an agentic analytics and workflow layer:
- Revenue cycle visibility improved with exception alerts surfacing denied or pending authorizations before they reached accounts receivable
- Operational decision-making accelerated as performance dashboards replaced manual reporting
- Identification of operational bottlenecks — including specific payers with systematic delay patterns — became possible at a level of granularity that was not previously available
- Leadership gained reliable, consistent performance tracking across programs
A geriatric care services provider operating across assisted living and long-term care settings achieved similar results, with particular gains in revenue leakage identification and service performance transparency — areas where manual prior authorization tracking had previously made root-cause analysis nearly impossible.
Cross-Setting Pattern: What These Deployments Have in Common
Across healthcare deployments, three outcomes appear consistently:
Faster authorization cycles. When intake, extraction, submission, and tracking are automated across all channels, the average time from authorization request to submission drops from days to hours. For urgent cases under the CMS 2026 mandate, this is not a convenience — it is a compliance requirement.
Lower denial rates. When submissions are assembled using complete clinical context — including unstructured data — and matched against current payer-specific criteria before submission, denials that stem from incomplete documentation or outdated criteria matching are largely eliminated.
Reduced operational overhead without reduced quality. Healthcare operations that deploy agentic AI for prior authorization consistently report that staff previously consumed by authorization follow-up tasks are redirected to higher-value work. Operations scale without proportional headcount increases — a critical factor as authorization volume continues to grow alongside expanding PA requirements.
Key Capabilities to Look for in an AI Prior Authorization Platform
Not all AI prior authorization platforms deliver equivalent outcomes. When evaluating options, these are the architectural and functional capabilities that separate genuinely agentic platforms from feature-enhanced point solutions.
Unified Context Engine: Structured and Unstructured Data Fusion
The platform must ingest and act on both structured data (EHR records, claims history, lab values) and unstructured data (clinical notes, PDF contracts, faxed referrals, policy documents, compliance memos). Platforms that only connect to structured sources will produce incomplete submissions and require human correction at scale.
Look for explicit support for Vision-LLM extraction, semantic document search, and real-time policy document ingestion — not just EHR API integration.
HIPAA, SOC 2, and Audit-Trail Governance Built In
In a regulated healthcare environment, compliance cannot be a layer added on top of a workflow tool. It must be built into the platform architecture. Evaluate for:
- HIPAA compliance with documented data handling and zero data retention policies
- SOC 2 Type II certification
- GDPR compliance for any cross-border data handling
- Role-based access controls on every agent action
- Immutable audit logs with full decision provenance, exportable for regulatory review
Platforms that offer compliance certifications but cannot demonstrate governance architecture at the system level are not suitable for prior authorization use cases in regulated environments.
EHR and Payer System Integrations at Scale
The platform should connect to your existing EHR, billing system, and payer portals without requiring data migration or system restructuring. Broad integration coverage — across 300+ enterprise systems — reduces deployment time and eliminates the siloed data problem that causes incomplete PA submissions.
Confirm that payer policy databases are updated continuously within the platform, not managed manually by your team.
Voice AI for Payer Follow-Up
A significant share of prior authorization delays occurs not during submission but during follow-up: calls to check status, respond to requests for additional information, and manage peer-to-peer review scheduling. Voice AI agents that can manage these calls autonomously — navigating payer IVR systems, documenting responses, and escalating to human staff when judgment is required — remove one of the highest-cost manual touchpoints in the PA workflow.
Healthcare teams using voice AI for payer follow-up have reported cutting administrative phone work by up to 60%.
Configurable Autonomy and Human-in-the-Loop Controls
Fully autonomous PA processing is appropriate for standard, low-complexity requests. Clinical edge cases, high-risk denials, and appeal preparation should always involve human review. The platform must support configurable autonomy limits — where you define which decisions the agent handles independently and which trigger a structured human handoff.
This is not just a safety feature. It is a requirement under state laws in Texas, Arizona, Maryland, and others that prohibit AI from being the sole basis for a medical necessity denial.
AI for Prior Authorization by Specialty
The core automation architecture applies across specialties, but implementation priorities vary.
Medical Prior Authorization (General)
Across general medical practices, the highest-volume PA categories are specialty referrals, advanced imaging (MRI, CT, PET), surgical procedures, and specialty medications. Agentic AI handles all of these through a unified workflow, with specialty-specific payer criteria libraries applied at the matching stage.
AI for Pharmacy Prior Authorization
Pharmacy prior authorization involves medication-specific criteria, step therapy requirements, and formulary tier navigation. AI agents integrated with pharmacy benefit manager (PBM) systems can check formulary status, identify step therapy history, and pre-populate the clinical justification for non-formulary or step-exception requests — reducing pharmacist intervention time substantially.
AI for Prior Authorization in Mental Health
Mental health prior authorization is among the most burdensome in the system, with payers frequently requesting extensive clinical documentation across multiple sessions before approving continued care. AI that can extract, summarize, and package multi-session clinical notes into structured PA submissions — and track approval timelines against mental health parity requirements — addresses a critical operational and compliance need.
AI Prior Authorization for Home Health and Staffing
Home health and staffing environments face layered authorization requirements: facility-level compliance, credential verification, payer-specific coverage rules, and visit-level authorization renewal. Agentic AI that integrates staffing coordination with authorization workflow — matching only credentialed, authorized staff to approved service requests — eliminates the coordination failures that drive compliance risk and unfilled service hours.
CMS 2026 Compliance: What You Need to Know Now
The CMS Interoperability and Prior Authorization Final Rule is not a future consideration. It is in effect.
What the rule requires:
- Covered health plans must respond to urgent PA requests within 72 hours
- Standard PA requests must receive a response within 7 business days
- Health plans must implement FHIR-based APIs to enable electronic PA data exchange
- Starting March 31, 2026, health plans must publicly report PA turnaround times, denial rates, appeal rates, and overturn rates
What this means for providers: Providers who can submit complete, accurate prior authorization requests electronically — and track responses in real time — will receive decisions faster and with fewer requests for additional information. Providers still relying on phone and fax submission will be at a systematic disadvantage as payer systems optimize for electronic workflows.
What this means for health plans: Plans that cannot demonstrate compliance with response time mandates will face public reporting scrutiny beginning this year. Plans that use AI to operationalize compliance — managing decision timelines, tracking overturn rates, and surfacing systematic denial patterns — will be better positioned than those attempting to meet mandates through manual process improvements.
What agentic AI enables specifically: Agentic AI platforms that maintain complete, timestamped audit logs of every PA submission and response give health plans and providers the documentation infrastructure to demonstrate compliance. Real-time status monitoring ensures that approaching response deadlines trigger automated alerts before they are breached — rather than after a complaint is filed.
How to Implement AI for Medical Prior Authorization in 4 Weeks
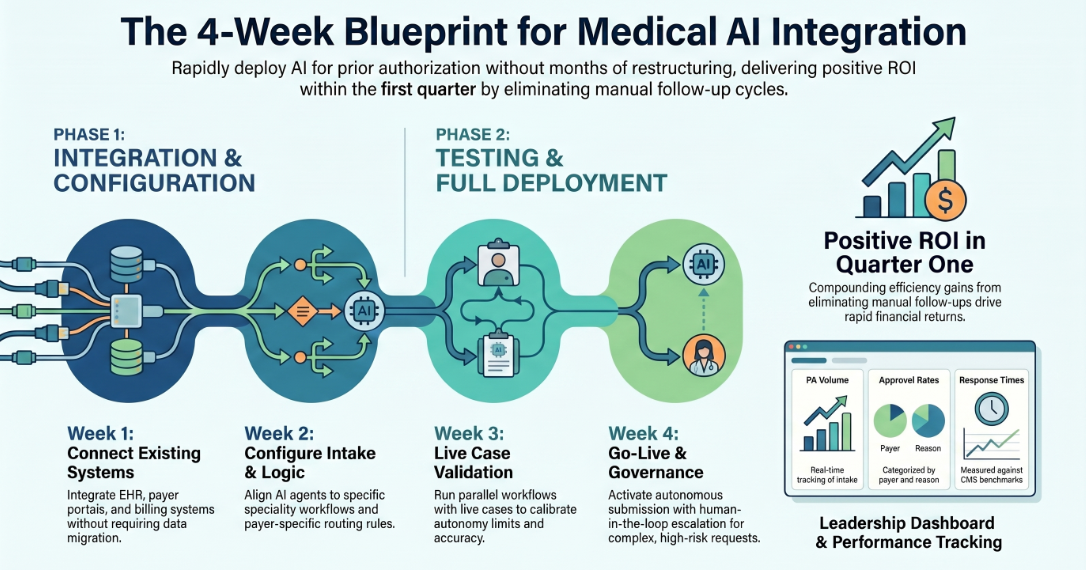
One of the most common barriers to AI adoption in healthcare operations is the assumption that implementation requires months of system restructuring. With a platform built to work with existing infrastructure rather than replace it, deployment timelines are significantly shorter than most operations teams expect.
Week 1: Connect Existing Systems
The platform integrates with your existing EHR, payer portals, billing system, and document management environment. No data migration is required. Integration is configured to your specific payer mix and specialty workflow. HIPAA compliance and access controls are activated at the point of connection.
Week 2: Configure Intake and Classification Agents
Intake channels are configured — email, fax, portal, voice, and any messaging platforms in use. Classification logic is aligned to your authorization categories and payer-specific routing rules. Clinical document extraction is tested against your document types, including any specialty-specific formats.
Week 3: Test with Live Prior Authorization Cases
The system runs in parallel with existing workflows, processing live PA cases and comparing agent-assembled submissions against current manual outputs. Accuracy is validated. Edge cases are identified and autonomy limits are calibrated. Staff complete a structured onboarding to the exception-handling and escalation interface.
Week 4: Go Live with Governance Controls Active
Full production deployment. The agent handles intake, extraction, submission, and tracking autonomously for standard cases. Human-in-the-loop escalation is active for complex and high-risk requests. Leadership dashboards surface real-time PA volume, approval rates, denial reasons, and response time performance against CMS benchmarks.
Most healthcare operations that deploy this way report positive ROI within the first quarter — driven by the compounding efficiency of eliminating manual follow-up cycles across hundreds or thousands of monthly PA requests.
The Bottom Line
Prior authorization is not going to get simpler. Payer requirements are expanding. CMS compliance mandates are now in effect. Authorization volume is increasing alongside growing PA requirements across specialties and settings.
The operations teams and health plans that will absorb this without proportional cost increases are the ones deploying agentic AI that handles the workflow end to end — not point tools that automate a single step and leave the coordination, exception handling, and follow-up to already-stretched staff.
The technology to do this exists today. The compliance pressure to act on it is immediate.
assistents.ai is the enterprise agentic AI platform built specifically for this kind of operational transformation. With HIPAA, SOC 2, GDPR, and ISO 27001 compliance built into the architecture, 300+ enterprise integrations, and a four-week deployment window, it is designed for healthcare operations that cannot afford a six-month implementation timeline.
The platform fuses structured and unstructured data through a three-tier Autonomy Stack — Unified Context Engine, Semantic Governor, and Active Orchestrator — giving AI agents complete clinical context before every prior authorization decision, with full audit provenance at every step.
If you are evaluating what it would take to move your prior authorization operations from manual workflows to autonomous, governed execution, the starting point is a live assessment of your specific workflows, payer mix, and compliance requirements mapped against what the platform delivers.
Book a demo with assistents.ai →
FAQS
What is AI for medical prior authorization?
AI for medical prior authorization refers to the use of artificial intelligence — and specifically agentic AI systems — to automate the process of obtaining insurance pre-approval for medical treatments, procedures, and medications. This includes intake capture, clinical data extraction, payer rule matching, electronic submission, status tracking, and exception management, replacing manual workflows that currently consume significant staff time and cause treatment delays.
How does AI help with prior authorization?
AI helps with prior authorization by automating each step of the workflow end to end. It extracts clinical information from structured and unstructured sources, matches patient data against current payer-specific criteria, assembles complete submission packages, submits electronically, tracks responses in real time, and escalates exceptions to human reviewers with full context. The result is faster approvals, fewer denials from incomplete submissions, and significantly reduced staff time on administrative follow-up.
Can AI reduce prior authorization denials?
Yes. Prior authorization denials most commonly result from incomplete documentation, incorrect coding, and failure to match current payer clinical criteria. AI addresses all three: it extracts complete clinical documentation including unstructured sources, applies current payer-specific rules at the point of submission, and flags gaps before a request is sent. Platforms operating with full clinical context architectures report prior authorization accuracy rates above 98% and denial rates below 2%.
What is the CMS prior authorization rule for 2026?
The CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F), effective January 1, 2026, requires covered health plans to respond to urgent prior authorization requests within 72 hours and standard requests within 7 business days. Beginning March 31, 2026, health plans must publicly report their PA turnaround times, denial rates, appeal rates, and overturn rates. The rule also requires FHIR-based API implementation to support electronic PA data exchange.
Is AI prior authorization HIPAA compliant?
AI prior authorization platforms built for enterprise healthcare deployments carry HIPAA compliance as a core architectural requirement, not an add-on. This includes zero data retention policies (enterprise data is not used for model training), role-based access controls, encrypted data handling, and immutable audit logs with full decision provenance. When evaluating platforms, verify HIPAA readiness is documented at the system architecture level, not only at the data transfer level.
How long does AI take for prior authorization approval?
AI-assisted prior authorization eliminates the submission-side delays that account for the majority of the current approval timeline. With automated intake, extraction, and electronic submission, a standard prior authorization can be assembled and submitted within minutes of a clinical order being placed. The remaining timeline depends on payer response speed — which the CMS 2026 mandate is now enforcing at 72 hours for urgent and 7 days for standard requests.
What is the difference between ePA and AI prior authorization?
Electronic Prior Authorization (ePA) refers to the digitization of the PA submission process — moving from phone and fax to electronic form submission. AI prior authorization goes further: it automates the clinical data extraction, payer criteria matching, submission assembly, and post-submission tracking that ePA systems still require humans to perform. AI prior authorization can be built on top of ePA infrastructure, but ePA alone does not automate the workflow.
What should I look for in an AI prior authorization platform?
The most important capabilities are: a unified context engine that processes both structured and unstructured clinical data; HIPAA, SOC 2, and audit-trail governance built into the platform architecture; broad EHR and payer integrations without requiring data migration; voice AI for payer follow-up calls; and configurable autonomy controls with human-in-the-loop escalation for complex cases. Platforms that automate only one or two steps in the workflow will not eliminate the operational burden — they will shift it.

Transform Your Business With Agentic Automation
Agentic automation is the rising star posied to overtake RPA and bring about a new wave of intelligent automation. Explore the core concepts of agentic automation, how it works, real-life examples and strategies for a successful implementation in this ebook.
Sarfraz Nawaz is the CEO and founder of Ampcome, which is at the forefront of Artificial Intelligence (AI) Development. Nawaz's passion for technology is matched by his commitment to creating solutions that drive real-world results. Under his leadership, Ampcome's team of talented engineers and developers craft innovative IT solutions that empower businesses to thrive in the ever-evolving technological landscape.Ampcome's success is a testament to Nawaz's dedication to excellence and his unwavering belief in the transformative power of technology.
More insights
Discover the latest trends, best practices, and expert opinions that can reshape your perspective





Contact us

