

AI Agents in Clinical Trials 2026: Use Cases, Real-World Results, and Your Deployment Roadmap




Clinical trials are the most expensive, slowest, and operationally fragile phase of the entire drug development process — and the vast majority of that friction has nothing to do with the science.
Between 2020 and 2024, average clinical trial cycle times increased by 14 months, even as the gap between individual trials shortened. Phase III trials now average nearly six million data points each — roughly three times the volume from a decade ago. Failed trials cost between $800 million and $1.4 billion per study. And the clinical research associates (CRAs) responsible for keeping trials on track are overwhelmed — manually monitoring dozens of siloed systems, managing data that no single person or team can synthesise fast enough, and spending more time on administrative tasks than on the work that actually matters.
AI agents are changing this. Not by replacing the humans in the room, but by removing the operational drag that has always slowed them down.
This guide covers exactly what AI agents do in clinical trials, where they are making the biggest impact, what real enterprise deployments look like, and how your organisation can go from evaluation to production — faster than you think.
What Are AI Agents in Clinical Trials?
Before looking at use cases, it helps to understand what distinguishes AI agents from the AI tools most healthcare and life sciences organisations have already encountered.
Traditional AI in clinical research tends to be narrow and passive. A machine learning model might flag anomalies in a dataset, or a rules engine might trigger a notification when a patient misses a check-in. These tools analyse and report. They do not act.
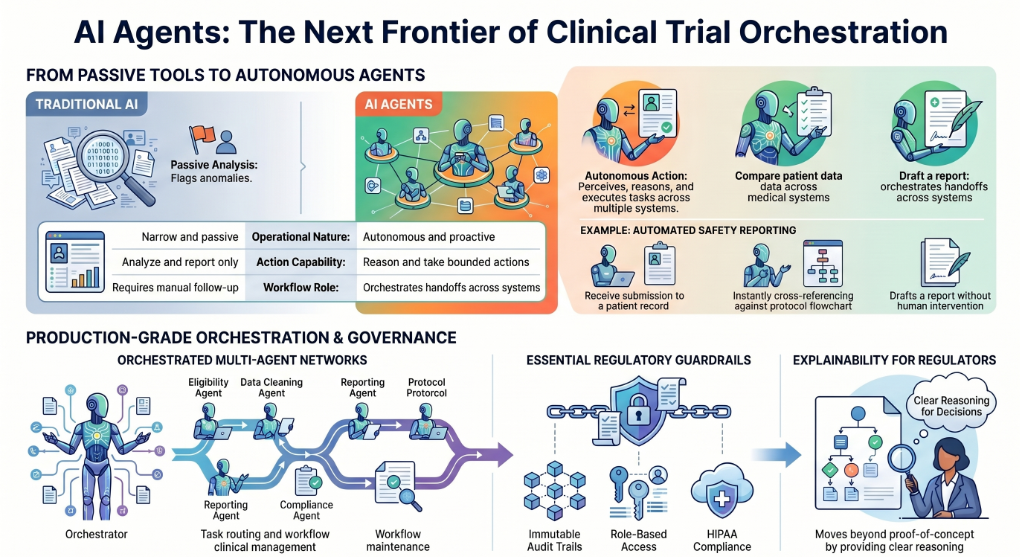
AI agents are different. An AI agent perceives context, reasons over it, makes bounded decisions, and takes actions — autonomously, across multiple systems, in sequence. A multi-agent system extends this further: a network of specialised agents, each with a defined role, coordinated by an orchestrator that routes tasks, manages handoffs, and maintains a coherent workflow across the entire trial pipeline.
In a clinical trial context, this means an AI agent can simultaneously monitor a patient's ePRO submissions, cross-reference them against protocol eligibility criteria, flag a potential adverse event, draft a safety report, and route it to the right team — without a human having to pull those threads together manually.
The key distinction is orchestration with governance. Any AI deployment in a regulated healthcare environment needs more than raw automation — it needs immutable audit trails, role-based access, explainability for regulators, and HIPAA compliance from day one. This is what separates a proof-of-concept from a production-grade system, and it is what Assistents is built to deliver.
Why Clinical Trials Need AI Agents Now
The operational crisis in clinical trials is not new. But it has accelerated to a point where traditional systems can no longer keep pace with the complexity being demanded of them.
The scale problem. The number of data points per Phase III trial has tripled over the past decade. Data flows in from EHRs, wearables, electronic patient-reported outcomes, lab systems, imaging platforms, CTMS, EDC systems, and more — all in real time, all requiring monitoring, all requiring reconciliation. No manual process can keep up with this volume reliably.
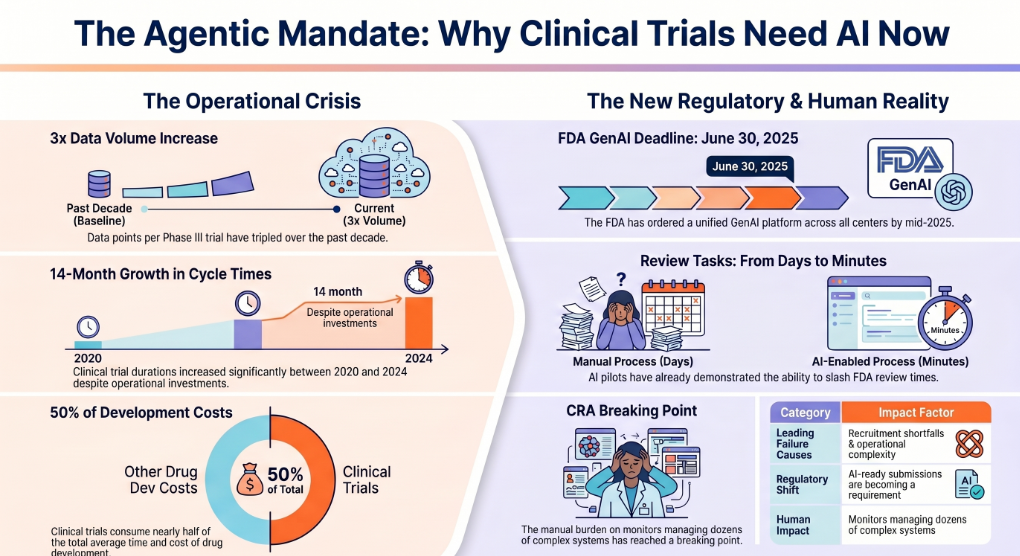
The time problem. Despite significant investment in operational improvement, clinical trial cycle times grew by 14 months between 2020 and 2024. Protocol deviations, recruitment shortfalls, site activation delays, and documentation backlogs are the primary culprits — and all of them are addressable with agentic automation.
The cost problem. Failed trials are catastrophically expensive. The inability to recruit the right patients in time and the absence of technology capable of managing operational complexity at scale remain the two leading causes of trial failure. Nearly half of the total average time and cost of drug development is consumed by clinical trials alone.
The regulatory pressure. Regulators are not standing still. Following a successful pilot in May 2025 in which AI cut certain FDA review tasks from days to minutes, the agency ordered a unified GenAI platform across all of its centres by June 30, 2025, and named a Chief AI Officer to govern it. For sponsors, this has a direct implication: submissions that are cleanly structured, machine-parsable, and consistent with emerging FDA guidance on AI-generated and AI-analysed data will move faster. AI-ready documents are no longer an advantage — they are becoming an expectation.
The human burden. CRAs are on the front line of all of this. They are responsible for monitoring increasingly complex trials across dozens of systems while maintaining data integrity and patient safety at every step. The manual burden has reached a breaking point, arriving — somewhat fatefully — at exactly the same moment that agentic AI has matured enough to offer a credible solution.
7 High-Impact Use Cases for AI Agents in Clinical Trials
1. Patient Recruitment and Eligibility Screening
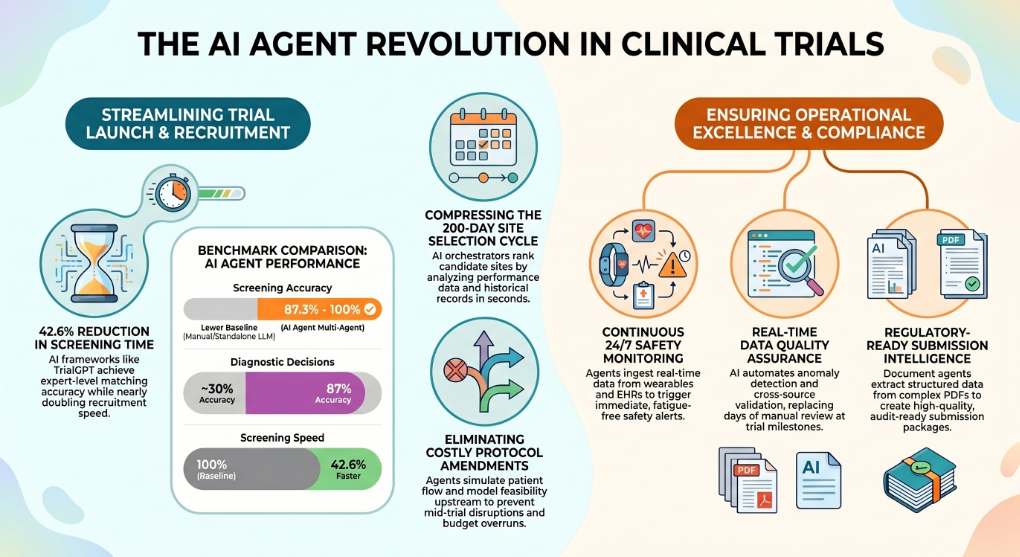
Patient recruitment is the single most common reason clinical trials run over time and over budget. Identifying eligible patients across fragmented healthcare systems, matching them to complex eligibility criteria, and doing it at the speed a competitive trial timeline demands — this is exactly where AI agents deliver immediate, measurable value.
Multi-agent systems built for patient matching can analyse EHR databases at scale, apply protocol-specific inclusion and exclusion criteria, rank candidates by fit, and surface a qualified recruitment list — continuously, as new patients enter the system. Research on large language model-based trial matching (specifically the TrialGPT framework) demonstrated criterion-level accuracy of 87.3%, nearly matching expert-level performance, while reducing screening time by 42.6%.
In operational oncology contexts, GPT-4-based agents with multimodal tool access have reached 87% accuracy in diagnostic and enrollment decisions — nearly tripling the performance of standalone LLMs used without an agentic framework. The MAKAR multi-agent framework achieved 100% accuracy in controlled patient-trial matching tasks by using role-specific agents to navigate complex eligibility criteria.
AI agents do not just find more patients faster. They find the right patients, with fewer false starts, and they do it without requiring a dedicated team to manually search and cross-reference patient databases.
2. Protocol Design and Optimisation
Protocol amendments are one of the largest hidden costs in clinical development. Each amendment introduces delays, increases site burden, and can compromise data integrity. The underlying cause is almost always the same: protocols are designed with incomplete visibility into historical trial performance, site capabilities, and patient population behaviour.
AI agents change this by operating upstream. Before a protocol is finalised, agents can analyse historical trial data across comparable studies, flag design elements that have historically caused amendment rates to spike, simulate patient flow under different eligibility criteria, and model recruitment feasibility by geography and site.
The result is a protocol that goes into execution with fewer unknowns and a lower likelihood of mid-trial disruption — which translates directly into faster timelines and lower costs.
3. Clinical Site Selection and Activation
Site selection and activation is one of the most time-consuming phases of clinical trial start-up. Traditionally, it requires teams to manually evaluate dozens of candidate sites across capability, patient volume, past trial performance, regulatory standing, and logistical fit. The process alone often takes around 200 days.
AI orchestrator agents can compress this dramatically. By building knowledge bases from site performance data, biomedical databases, and historical trial records, agents can score and rank candidate sites, extract critical protocol-specific criteria, and surface the most viable options — in a fraction of the time a manual process requires. The orchestrator directs sub-agents in phased steps, allowing research teams to focus on final decisions rather than data assembly.
4. Real-Time Patient Monitoring and Adverse Event Detection
Patient safety monitoring is a continuous, multi-system obligation across every active trial. Missed signals — whether from a wearable device, a patient-reported outcome, or a lab result — can have serious consequences, both for patient safety and for data integrity.
AI agents operate on a continuous monitoring model that no human team can replicate. They ingest data in real time from EHRs, ePROs, wearables, laboratory systems, and operational platforms, apply protocol-defined safety rules, detect anomalies and deviations, and trigger the appropriate response workflow — automatically, with a full audit trail.
This is not just faster than manual monitoring. It is more consistent. Agents do not have cognitive fatigue, do not miss a data point because a system was not checked, and do not require shift handoffs.
Assistents deploys autonomous agent layers that connect to existing trial data infrastructure and monitor for safety signals continuously, with configurable alerting and escalation logic built in from day one.
5. Clinical Data Management and Quality Assurance
The volume and heterogeneity of clinical trial data — spanning genomics, EHRs, wearables, imaging, and operational systems — makes consistent data quality one of the hardest problems in research operations. Ensuring that data is complete, consistent, and compliant across all integrated sources is a full-time job for large data management teams.
AI agents automate the routine but critical tasks that consume that team's capacity: validating incoming data against protocol rules, detecting anomalies and missing values, flagging discrepancies between integrated sources, and maintaining a consistent quality standard across the entire dataset in real time.
What typically takes days of data review at a trial milestone can happen continuously, in the background, with issues surfaced immediately rather than discovered weeks later during a data lock.
6. Regulatory Documentation and Submission Support
Regulatory documentation is where the consequences of operational inefficiency are most acutely felt. Submission packages require the synthesis of data from dozens of sources into structured, consistent, machine-parsable documents — and the FDA's increasingly AI-enabled review process means that document quality now directly affects review speed.
AI agents built for document intelligence can extract structured data from complex PDFs and clinical reports, draft regulatory-ready content against predefined templates, maintain traceability across source data and submission claims, and generate the audit artifacts that regulators increasingly expect.
The shift here is significant. Sponsors who invest in AI-ready document workflows today will have a structural advantage as the FDA's own AI review infrastructure matures — because their submissions will be the ones that move fastest through an increasingly automated review pipeline.
This is a capability area where Assistents has deployed document intelligence agents in production environments — systems that handle intelligent document ingestion, multi-agent extraction from complex PDFs, and full audit logging — with measurable improvements in processing accuracy and turnaround time.
7. Patient Engagement and Retention
Participant dropout is a persistent problem that derails recruitment timelines and compromises statistical power. The operational causes are often straightforward: missed reminders, unanswered questions, logistical friction, and a lack of consistent communication across the trial duration.
AI voice agents and conversational agents address these causes directly. They handle appointment reminders, consent renewals, check-in prompts, and participant queries — 24 hours a day, in the participant's preferred language, at whatever communication channel they use most.
This is not a replacement for the clinical relationship. It is the operational infrastructure that supports it — ensuring participants have what they need, when they need it, without requiring a coordinator to manually manage every touchpoint.
Assistents' voice AI agents are deployed in healthcare operations with multi-language support, configurable voice and persona, and full integration with scheduling and EHR systems — making them ready to drop into patient engagement workflows immediately.
Real-World Results: What Enterprise Deployments Look Like
The most important thing to understand about AI agents in healthcare is that the results being discussed are not hypothetical projections. They are live production deployments, delivering measurable outcomes for healthcare organisations right now.
Here is what real deployments look like, drawn from Assistents' production client base:
Healthcare Staffing and Workforce Operations
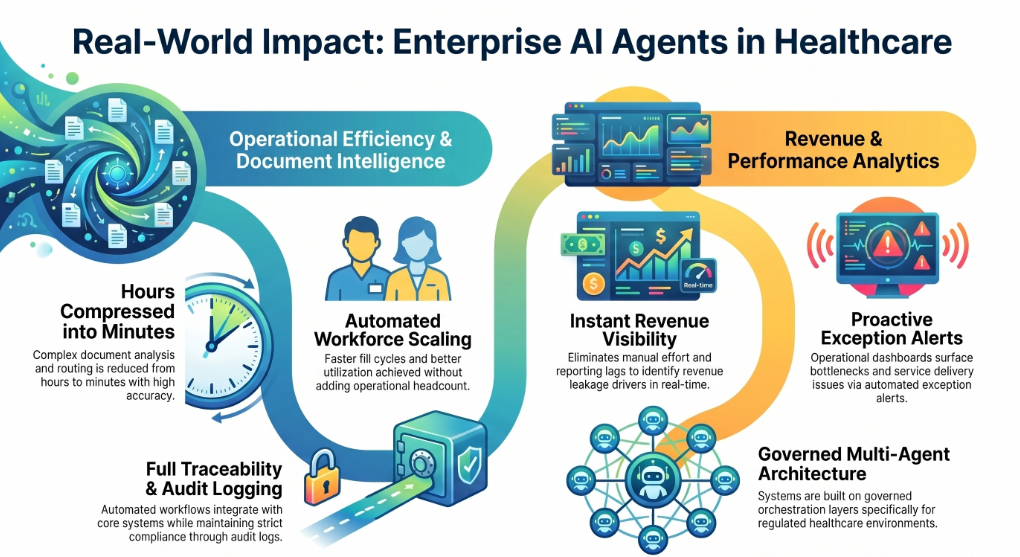
A healthcare staffing platform deployed AI agents to automate matching, scheduling, and compliance workflows across a high-volume operation connecting clinical professionals with healthcare facilities. The results included faster fill cycles, lower scheduling friction, better workforce utilisation, and improved staffing responsiveness for facilities — all without adding operational headcount. The system also delivered reporting on fill rates and utilisation, giving leadership real-time visibility into a previously opaque operation.
Inpatient Care Revenue and Operational Analytics
A physician-led clinical enterprise with deep roots in inpatient care deployed analytics agents to unify revenue and operational performance data. Before deployment, leadership visibility into revenue performance required significant manual effort and lagged by days. After deployment, the organisation achieved faster identification of revenue leakage drivers, more reliable performance tracking, and unified reporting that surfaced operational bottlenecks in real time. Analytics agents also improved billing workflow visibility and reduced the time required to act on recurring operational questions.
Geriatric and Long-Term Care Performance Management
A geriatric care services provider deployed operational and revenue analytics agents to improve performance visibility across assisted living and long-term care programs. The deployment delivered program operations dashboards, staffing and service delivery analytics, and revenue cycle visibility with exception alerts — giving leadership better decision support and faster identification of operational bottlenecks. The system is designed to improve transparency into service performance in an environment where margin management and care quality are both mission-critical.
Document Intelligence in Healthcare Operations
In environments where complex documents — clinical protocols, compliance materials, procurement records — need to be ingested, analysed, and routed at speed, Assistents has deployed multi-agent document workbenches that achieve high extraction accuracy targets for standard formats, detect revisions and changes, and integrate with core operational systems with full audit logging. What previously required hours of manual processing is compressed into minutes, with fewer errors and full traceability.
These deployments share a common architecture: they are built on governed, orchestrated, multi-agent systems — not point-solution AI tools. The governance layer is what makes them production-ready for regulated healthcare environments.
The Architecture Behind AI Agents in Clinical Trials
For clinical trial deployments to work at scale, the underlying architecture matters as much as the AI itself. Here is the foundational structure that makes agentic AI reliable in a regulated clinical environment:
Data Ingestion Layer
Connects to all relevant trial data sources — EHRs, EDC systems, CTMS, ePRO platforms, wearables, laboratory systems, and imaging platforms. Handles structured and unstructured data, with quality checks at the point of ingestion.
Builds a coherent, protocol-aligned representation of each patient, site, and trial operation from across all connected sources. This is the foundation that agents reason over — without it, agentic outputs are only as good as whichever data source an agent happens to query first.
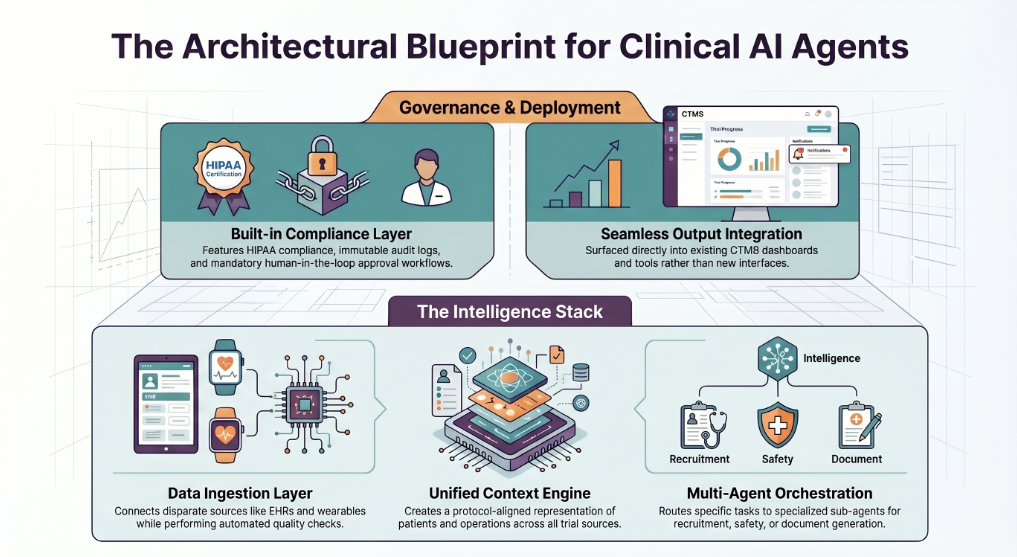
Multi-Agent Orchestration Layer
A coordinating orchestrator routes tasks to specialised sub-agents based on context and urgency. Each sub-agent has a defined role — recruitment screening, safety monitoring, document generation, data quality — and operates within a governed set of decision rules. The orchestrator maintains coherence across the workflow and manages handoffs between agents.
Governance and Compliance Layer
HIPAA compliance, immutable audit logs, role-based access controls, explainability artifacts for regulatory review, and configurable approval workflows for decisions that require human sign-off. This layer is not an add-on — it is built into the architecture from the start.
Output and Integration Layer
Agents surface their outputs into the systems teams already use — CTMS dashboards, safety reporting platforms, document management systems, CRM, and communication tools — rather than requiring teams to log into a new interface.
This architecture is what distinguishes a system that can operate in production, under regulatory scrutiny, from a demonstration environment.
Regulatory Compliance and AI Governance in Clinical Trials
Regulatory compliance is not a constraint on AI deployment in clinical trials — it is a design requirement. Any AI agent operating in a clinical trial environment must be built with this assumption from the beginning.
The FDA's direction is clear. Following its 2025 AI pilot, the agency is moving toward a review environment in which submissions that are machine-parsable, consistently structured, and accompanied by clear data lineage and validation artifacts will move faster through review. This creates a direct incentive for sponsors to align their AI deployments with emerging FDA guidance on AI-generated and AI-analysed data.
The practical implications for your AI agent deployment include:
21 CFR Part 11 compliance. Any AI system that creates, modifies, or transmits electronic records in a clinical trial context must comply with Part 11 requirements for electronic signatures, audit trails, and system validation.
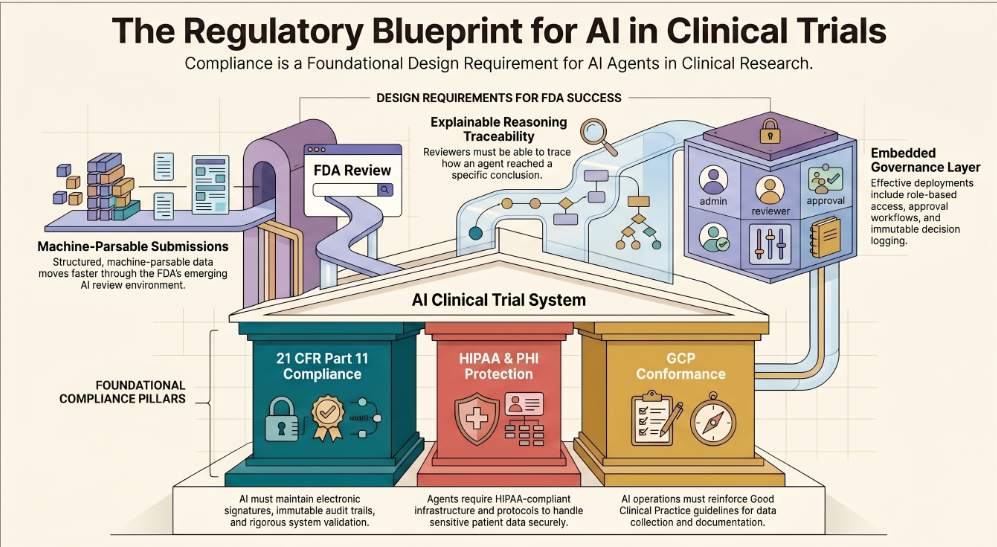
HIPAA alignment. AI agents that access, process, or store patient data require HIPAA-compliant infrastructure, Business Associate Agreements, and data handling protocols that meet PHI protection standards.
GCP conformance. Good Clinical Practice guidelines govern how data is collected, processed, and documented across clinical trials. AI agents must operate within — and reinforce — these standards, not circumvent them.
Explainability and traceability. Regulatory reviewers need to be able to trace how an AI agent reached a conclusion or generated an output. This requires that agent reasoning, data sources, and decision logic are logged in a form that can be reviewed and audited.
Assistents' platform is built with all of these requirements embedded. Every agent deployment includes immutable audit logging, role-based access control, configurable approval workflows for decisions above a defined confidence threshold, and a governance layer that enforces consistent decision logic across all agents.
How to Deploy AI Agents in Clinical Trials: A Step-by-Step Roadmap
One of the most common misconceptions about AI agent deployment in clinical settings is that it requires a long, expensive, high-risk implementation. The reality for organisations working with the right platform is very different.
Here is a practical roadmap:
Step 1: Define a high-friction, high-value use case. Do not start with the broadest possible vision. Start with the workflow that is causing the most operational pain right now. Patient recruitment screening, adverse event monitoring, and site performance reporting are common starting points — each delivers measurable value quickly and creates a foundation for broader deployment.
Step 2: Audit your data infrastructure. Identify where the relevant data lives — which EHR systems, CTMS platforms, and operational tools are in scope — and assess data quality, access controls, and integration readiness. The quality of your agentic outputs will be bounded by the quality of your data inputs.
Step 3: Establish governance requirements. Define the approval workflows, audit trail requirements, escalation logic, and compliance obligations that apply to your deployment. For any decision that affects patient safety or regulatory records, define the human-in-the-loop checkpoints explicitly.
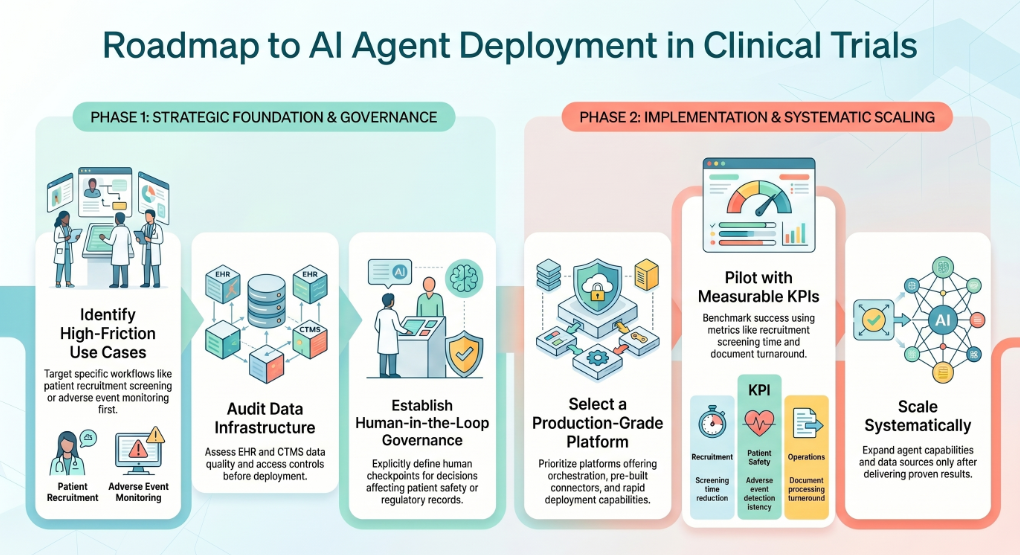
Step 4: Select a production-grade platform. Look for a platform that handles orchestration, governance, and integration as core capabilities — not afterthoughts. The ability to deploy quickly without sacrificing auditability is the key differentiator. Assistents deploys production AI agents in healthcare environments in under three weeks, with pre-built connectors for major EHR, CTMS, and operational platforms.
Step 5: Pilot with measurable success criteria. Define the KPIs before you start: recruitment screening time, data quality rate, adverse event detection latency, document processing turnaround. Run a time-bounded pilot against these metrics. Real results from a defined scope are more valuable than a large-scale rollout without benchmarks.
Step 6: Scale systematically. Once the initial use case is in production and delivering results, expand methodically — adding data sources, agent capabilities, and use cases in a sequence that maintains governance standards and does not outpace your team's ability to manage the system.
The Bottom Line
Clinical trials have always demanded extraordinary precision. The operational infrastructure supporting them has not kept pace with the complexity that precision now requires.
AI agents close that gap. They do not change the science — they remove the operational drag that has been slowing it down: the manual data aggregation, the fragmented monitoring, the documentation backlogs, the recruitment delays, the reporting overhead that consumes the bandwidth of people who should be focused on what happens to patients.
The organisations that deploy AI agents in clinical trial operations today are not taking a risk on emerging technology. They are making a structural choice to operate faster, with better data quality, with stronger regulatory compliance, and with a human team that is freed to do the work that actually requires human judgement.
Assistents deploys production-grade, governed, multi-agent AI systems for healthcare and life sciences organisations — from patient recruitment to regulatory documentation to operational analytics. Most deployments go live in under three weeks.
If you are ready to see what this looks like for your trial operations, book a demo with the Assistents team — or explore our Healthcare AI Agent solutions to see the full platform.
FAQs
What is the role of AI agents in clinical trials?
AI agents automate the operational workflows that consume the most time and introduce the most risk in clinical trial management — including patient recruitment, real-time safety monitoring, data quality management, regulatory documentation, and site performance tracking. Unlike traditional AI tools that analyse and report, AI agents take action: they perceive context, make bounded decisions, and execute tasks across multiple systems autonomously and in sequence.
How are AI agents different from traditional AI in clinical research?
Traditional AI in clinical research is typically narrow, passive, and task-specific — a model flags an anomaly, and a human decides what to do with that information. AI agents are active: they perceive, reason, act, and coordinate across multiple systems and workflows. Multi-agent systems add a coordination layer, enabling networks of specialised agents to manage complex, multi-step processes end-to-end.
Can AI agents replace CRAs in clinical trials?
No — and the best AI agent deployments are not designed to. The role of a CRA in maintaining data integrity, managing site relationships, and exercising clinical judgement is not replaceable by an AI system. What AI agents replace is the administrative burden that has been degrading CRAs' ability to do that work effectively: manual data aggregation, cross-system monitoring, documentation drafting, and routine reporting.
What are the best AI platforms for clinical trial management?
Production-grade platforms for clinical trial AI should offer multi-agent orchestration, not just single-model tools. The key criteria are: HIPAA compliance and regulatory governance built in by design, integration readiness with existing EHR and CTMS systems, explainability and audit trail capabilities, and the ability to move from pilot to production without a multi-year implementation. Assistents meets all of these criteria and deploys in under three weeks.
How does agentic AI help with patient recruitment in clinical trials?
Agentic AI helps patient recruitment by continuously screening patient databases against protocol-specific eligibility criteria, ranking candidates by match quality, flagging eligible patients as they enter the system, and managing outreach workflows — all automatically and at a scale that no manual process can match. Research frameworks have demonstrated screening time reductions of over 40% with accuracy levels approaching expert-level clinical judgement.
Is AI in clinical trials FDA-compliant?
AI can be deployed in clinical trials in a fully FDA-compliant manner, provided the deployment is designed with regulatory requirements embedded from the start. This includes 21 CFR Part 11 compliance for electronic records, HIPAA-aligned data handling, GCP conformance, and the ability to produce explainability artifacts and audit trails that meet regulatory review standards. The FDA itself is actively implementing AI in its own review processes and has signalled that AI-ready submissions will move faster through review.
What are the risks of using AI in clinical trials?
The primary risks include data quality issues producing unreliable outputs, lack of explainability making regulatory review difficult, compliance gaps creating regulatory exposure, and over-automation in areas where human judgement is essential for patient safety. These risks are all mitigable through proper platform selection, governance design, and human-in-the-loop checkpoints at defined decision boundaries. The risk of not using AI — falling further behind on trial timelines and operational efficiency — is increasingly the greater risk for most organisations.
How long does it take to deploy AI agents in a clinical trial environment?
With a governed, production-grade platform, the timeline from scoping to live deployment for an initial use case is typically under three weeks. This assumes clear data access, defined governance requirements, and integration readiness for the target systems. Assistents has deployed production healthcare AI agent systems within this timeframe across multiple healthcare and life sciences clients.

Transform Your Business With Agentic Automation
Agentic automation is the rising star posied to overtake RPA and bring about a new wave of intelligent automation. Explore the core concepts of agentic automation, how it works, real-life examples and strategies for a successful implementation in this ebook.
Sarfraz Nawaz is the CEO and founder of Ampcome, which is at the forefront of Artificial Intelligence (AI) Development. Nawaz's passion for technology is matched by his commitment to creating solutions that drive real-world results. Under his leadership, Ampcome's team of talented engineers and developers craft innovative IT solutions that empower businesses to thrive in the ever-evolving technological landscape.Ampcome's success is a testament to Nawaz's dedication to excellence and his unwavering belief in the transformative power of technology.
More insights
Discover the latest trends, best practices, and expert opinions that can reshape your perspective






.webp)
Contact us

